Nkechi Anne Enechukwu MBBS, FMCP (Derm), Gabriel Olabiyi Ogun MBBS, FMCP (Pathology)
{"title":"Dermoscopic clues of dermatitis cruris pustulosa et atrophicans: A distinct folliculitis in dark skin phototypes","authors":"Nkechi Anne Enechukwu MBBS, FMCP (Derm), Gabriel Olabiyi Ogun MBBS, FMCP (Pathology)","doi":"10.1002/jvc2.467","DOIUrl":null,"url":null,"abstract":"<p>Dermatitis cruris pustulosa et atrophicans (DCPA) is a chronic folliculitis prevalent in tropical regions, marked by intensely pruritic recurring follicular pustules with cutaneous oedema, subsequently followed by alopecia, and atrophy of the affected areas. It predominantly affects the shin, exhibits frequent relapses and often displays a limited response to therapy. Despite being described initially as the “Nigerian shin disease,” it has been reported from various continents.<span><sup>1-3</sup></span></p><p>Dermoscopy, an evolving diagnostic tool in the dark skin, has demonstrated high diagnostic utility in various forms of folliculitis; however, its application in DCPA remains unexplored, creating a gap in the literature.<span><sup>4</sup></span> Given that several other forms of folliculitis prevalent in the tropics mimic DCPA, elucidating the distinctive dermoscopic features of DCPA is essential to enhance diagnostic accuracy and differentiate it from mimics.<span><sup>4</sup></span> We report a case of DCPA in the dark skin highlighting its dermoscopic features.</p><p>A 21-year-old female of African descent presented with a 6-year history of recurrent intensely pruritic right shin rashes. They started as papules and vesicles which became scaly, and occasionally, painful. She had atopic dermatitis and a notable habit of using petrolatum-based emollients for dry scaly skin. Examination revealed shiny right shin with sharply demarcated hyperpigmented areas harbouring multiple papules, vesicles, a few pustules. There was evident alopecia over these areas (Figure 1a).</p><p>Dermoscopy demonstrated an accentuated honeycomb pigment pattern, absent skin furrows, perifollicular pustules with coarse hairs emerging from their centres, absent pin point white dots (eccrine duct openings), substantial hair follicle depletion, perifollicular red areas, and areas exhibiting erosions. (Figure 1b–d). Posttreatment showed clearance of pustules and erythema. (Figure 1e,f).</p><p>Histopathology (40×) (Figure 2a,b) show mainly intense lymphocytic and few plasma cell infiltration around the hair follicles and other adnexial structures. The lymphoplamacytic infiltration extends from the supercial to deep dermis. There is associated perifollicular fibrosis. A diagnosis of DCPA was made.</p><p>She was treated with Co-trimoxazole and advised to avoid occlusive skin care products. Two months later, the lesion had improved with symptom resolution. (Figure 1e,f)</p><p>DCPA is uniquely localised to the shin, with rare occurrences on the forearms, trunk, and pubic area, exhibiting a preference for areas with terminal hairs.<span><sup>1-3</sup></span> Recurrent symmetric follicular pustules at the initial phase eventually progress to alopecia and atrophy of the affected area. Although characteristic, diagnosis can be challenging due to its rarity and resemblance to folliculitis of other aetiologies.</p><p>Dermoscopy, is potentially valuable for differentiating DCPA from other forms of folliculitis.<span><sup>4</sup></span> Perifollicular pustules suggests folliculitis, while associated ingrown hair indicates pseudofolliculitis. The hang-glider sign and serpiginous tracts indicate scabietic folliculitis. Fungal folliculitis is marked by broken, zigzag, morse code, and corkscrew hairs. Central round pustules with peripheral sparse dotted vessels, though diagnostically less accurate, suggests bacterial folliculitis. Demodex tails (creamy or whitish gelatinous follicular plugs protruding from follicular openings) and round creamy or whitish plugs surrounded by an erythematous halo indicate demodex folliculitis.<span><sup>4</sup></span> Peripheral, regularly distributed dotted vessels, in the absence of other findings, strongly indicate Malassezia folliculitis. Folliculitis decalvans typically presents with hair tufts.<span><sup>4</sup></span> Specifically, the loss of hair follicular and eccrine openings and presence of hair casts as seen in our patient are more indicative of DCPA.<span><sup>3, 5</sup></span> Exaggerated or discontinuous honey comb pigmentation and loss of normal skin furrows as was seen in our patient are nonspecific findings, and may be observed in other chronic inflammatory conditions in the dark skin.<span><sup>6</sup></span></p><p>Despite its rarity, further research is required, involving a larger sample of DCPA cases, to investigate the robustness of these features in distinguishing DCPA from other forms of folliculitis. An improved understanding of these dermoscopic features will lead to early diagnosis and reduced need for biopsies.</p><p>Nkechi Anne Enechukwu was involved in conceptualisation, methodology, writing—Original Draft Preparation, writing—Review and editing and visualisation. Gabriel Olabiyi Ogun was involved in Conceptualisation, writing—Original Draft Preparation, writing—Review and editing, supervision, investigation and Visualisation.</p><p>The authors' have no conflict of interest to declare.</p><p>The patient in this manuscript gave a written informed consent for participation in the study and the use of her deidentified, anonymized, aggregated data and their case details (including photographs) for publication. Ethical Approval: not applicable.</p>","PeriodicalId":94325,"journal":{"name":"JEADV clinical practice","volume":"3 3","pages":"920-922"},"PeriodicalIF":0.0000,"publicationDate":"2024-05-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jvc2.467","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JEADV clinical practice","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jvc2.467","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Dermatitis cruris pustulosa et atrophicans (DCPA) is a chronic folliculitis prevalent in tropical regions, marked by intensely pruritic recurring follicular pustules with cutaneous oedema, subsequently followed by alopecia, and atrophy of the affected areas. It predominantly affects the shin, exhibits frequent relapses and often displays a limited response to therapy. Despite being described initially as the “Nigerian shin disease,” it has been reported from various continents.1-3
Dermoscopy, an evolving diagnostic tool in the dark skin, has demonstrated high diagnostic utility in various forms of folliculitis; however, its application in DCPA remains unexplored, creating a gap in the literature.4 Given that several other forms of folliculitis prevalent in the tropics mimic DCPA, elucidating the distinctive dermoscopic features of DCPA is essential to enhance diagnostic accuracy and differentiate it from mimics.4 We report a case of DCPA in the dark skin highlighting its dermoscopic features.
A 21-year-old female of African descent presented with a 6-year history of recurrent intensely pruritic right shin rashes. They started as papules and vesicles which became scaly, and occasionally, painful. She had atopic dermatitis and a notable habit of using petrolatum-based emollients for dry scaly skin. Examination revealed shiny right shin with sharply demarcated hyperpigmented areas harbouring multiple papules, vesicles, a few pustules. There was evident alopecia over these areas (Figure 1a).
Dermoscopy demonstrated an accentuated honeycomb pigment pattern, absent skin furrows, perifollicular pustules with coarse hairs emerging from their centres, absent pin point white dots (eccrine duct openings), substantial hair follicle depletion, perifollicular red areas, and areas exhibiting erosions. (Figure 1b–d). Posttreatment showed clearance of pustules and erythema. (Figure 1e,f).
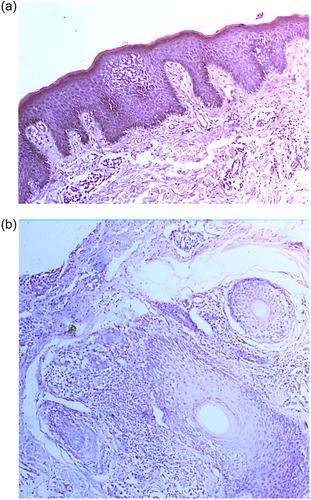
Histopathology (40×) (Figure 2a,b) show mainly intense lymphocytic and few plasma cell infiltration around the hair follicles and other adnexial structures. The lymphoplamacytic infiltration extends from the supercial to deep dermis. There is associated perifollicular fibrosis. A diagnosis of DCPA was made.
She was treated with Co-trimoxazole and advised to avoid occlusive skin care products. Two months later, the lesion had improved with symptom resolution. (Figure 1e,f)
DCPA is uniquely localised to the shin, with rare occurrences on the forearms, trunk, and pubic area, exhibiting a preference for areas with terminal hairs.1-3 Recurrent symmetric follicular pustules at the initial phase eventually progress to alopecia and atrophy of the affected area. Although characteristic, diagnosis can be challenging due to its rarity and resemblance to folliculitis of other aetiologies.
Dermoscopy, is potentially valuable for differentiating DCPA from other forms of folliculitis.4 Perifollicular pustules suggests folliculitis, while associated ingrown hair indicates pseudofolliculitis. The hang-glider sign and serpiginous tracts indicate scabietic folliculitis. Fungal folliculitis is marked by broken, zigzag, morse code, and corkscrew hairs. Central round pustules with peripheral sparse dotted vessels, though diagnostically less accurate, suggests bacterial folliculitis. Demodex tails (creamy or whitish gelatinous follicular plugs protruding from follicular openings) and round creamy or whitish plugs surrounded by an erythematous halo indicate demodex folliculitis.4 Peripheral, regularly distributed dotted vessels, in the absence of other findings, strongly indicate Malassezia folliculitis. Folliculitis decalvans typically presents with hair tufts.4 Specifically, the loss of hair follicular and eccrine openings and presence of hair casts as seen in our patient are more indicative of DCPA.3, 5 Exaggerated or discontinuous honey comb pigmentation and loss of normal skin furrows as was seen in our patient are nonspecific findings, and may be observed in other chronic inflammatory conditions in the dark skin.6
Despite its rarity, further research is required, involving a larger sample of DCPA cases, to investigate the robustness of these features in distinguishing DCPA from other forms of folliculitis. An improved understanding of these dermoscopic features will lead to early diagnosis and reduced need for biopsies.
Nkechi Anne Enechukwu was involved in conceptualisation, methodology, writing—Original Draft Preparation, writing—Review and editing and visualisation. Gabriel Olabiyi Ogun was involved in Conceptualisation, writing—Original Draft Preparation, writing—Review and editing, supervision, investigation and Visualisation.
The authors' have no conflict of interest to declare.
The patient in this manuscript gave a written informed consent for participation in the study and the use of her deidentified, anonymized, aggregated data and their case details (including photographs) for publication. Ethical Approval: not applicable.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


