Shadi P Bagherzadeh, Bettia E Celestin, Everton J Santana, Michael Salerno, Kari C Nadeau, Andrew J Sweatt, Roham T Zamanian, Francois Haddad
{"title":"Novel Reference Equations for Pulmonary Artery Size and Pulsatility Using Echocardiography and Their Diagnostic Value in Pulmonary Hypertension.","authors":"Shadi P Bagherzadeh, Bettia E Celestin, Everton J Santana, Michael Salerno, Kari C Nadeau, Andrew J Sweatt, Roham T Zamanian, Francois Haddad","doi":"10.1016/j.chest.2024.06.3805","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>According to the most recent pulmonary hypertension (PH) guidelines, a main pulmonary artery (MPA) diameter > 25 mm on transthoracic echocardiography supports the diagnosis of PH. However, the size of the pulmonary artery (PA) may vary according to body size, age, and cardiac phases.</p><p><strong>Research question: </strong>(1) What are the reference limits for PA size on transthoracic echocardiography, considering differences in body size, sex, and age? (2) What is the diagnostic value of the PA size for classifying PH? (3) How does the selection of different reference groups (healthy volunteers vs patients referred for right heart catheterization [RHC]) influence the diagnostic OR (DOR)?</p><p><strong>Study design and methods: </strong>The study included a reference cohort of 248 healthy individuals as control patients, 693 patients with PH proven by RHC, and 156 patients without PH proven by RHC. In the PH cohort, 300 had group 1 PH, 207 had group 2 PH, and 186 had group 3 PH. MPA and right PA diameters and areas were measured in the upper sternal short-axis and suprasternal notch views. Reference limits (5th-95th percentile) were based on absolute values and height-indexed measures. Quantile regression analysis was used to derive median and 95th quantile reference equations for the PA measures. DORs and probability diagnostic plots for PH were then determined using healthy control and non-PH cohorts.</p><p><strong>Results: </strong>The 95th percentile for indexed MPA diameter was 15 mm/m in diastole and 19 mm/m in systole in both sexes. Quantile regression analysis revealed a weak age effect (pseudo-R<sup>2</sup> of 0.08-0.10 for MPA diameters). Among measures, the MPA size in diastole had the highest DOR (156.2; 95% CI, 68.3-357.5) for detection of group 1 PH. Similarly, the DORs were also high for groups 2 and 3 PH when compared with the control cohort but significantly lower compared with the non-PH cohort.</p><p><strong>Interpretation: </strong>This study presents novel reference limits for MPA based on height indexing and quantile regression.</p>","PeriodicalId":9782,"journal":{"name":"Chest","volume":" ","pages":"1184-1196"},"PeriodicalIF":8.6000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11638547/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chest","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.chest.2024.06.3805","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/25 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: According to the most recent pulmonary hypertension (PH) guidelines, a main pulmonary artery (MPA) diameter > 25 mm on transthoracic echocardiography supports the diagnosis of PH. However, the size of the pulmonary artery (PA) may vary according to body size, age, and cardiac phases.
Research question: (1) What are the reference limits for PA size on transthoracic echocardiography, considering differences in body size, sex, and age? (2) What is the diagnostic value of the PA size for classifying PH? (3) How does the selection of different reference groups (healthy volunteers vs patients referred for right heart catheterization [RHC]) influence the diagnostic OR (DOR)?
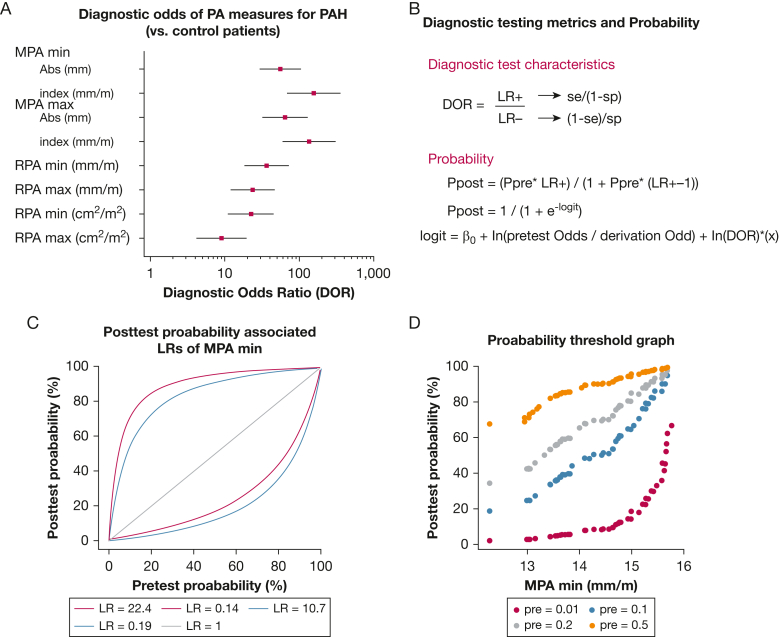
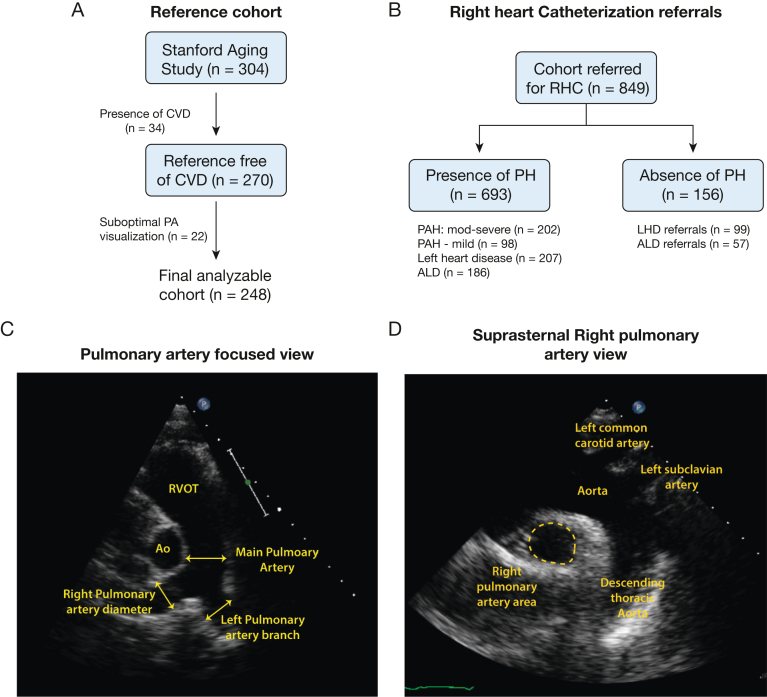
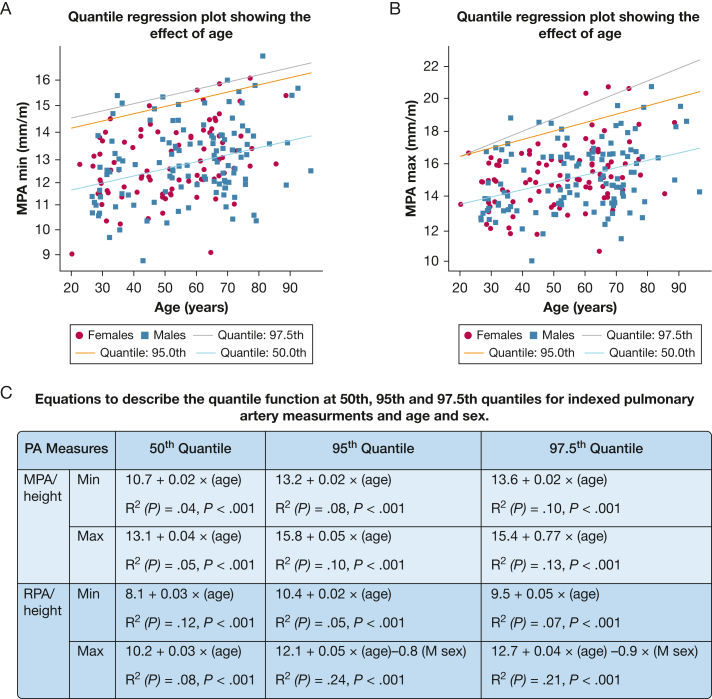
Study design and methods: The study included a reference cohort of 248 healthy individuals as control patients, 693 patients with PH proven by RHC, and 156 patients without PH proven by RHC. In the PH cohort, 300 had group 1 PH, 207 had group 2 PH, and 186 had group 3 PH. MPA and right PA diameters and areas were measured in the upper sternal short-axis and suprasternal notch views. Reference limits (5th-95th percentile) were based on absolute values and height-indexed measures. Quantile regression analysis was used to derive median and 95th quantile reference equations for the PA measures. DORs and probability diagnostic plots for PH were then determined using healthy control and non-PH cohorts.
Results: The 95th percentile for indexed MPA diameter was 15 mm/m in diastole and 19 mm/m in systole in both sexes. Quantile regression analysis revealed a weak age effect (pseudo-R2 of 0.08-0.10 for MPA diameters). Among measures, the MPA size in diastole had the highest DOR (156.2; 95% CI, 68.3-357.5) for detection of group 1 PH. Similarly, the DORs were also high for groups 2 and 3 PH when compared with the control cohort but significantly lower compared with the non-PH cohort.
Interpretation: This study presents novel reference limits for MPA based on height indexing and quantile regression.
期刊介绍:
At CHEST, our mission is to revolutionize patient care through the collaboration of multidisciplinary clinicians in the fields of pulmonary, critical care, and sleep medicine. We achieve this by publishing cutting-edge clinical research that addresses current challenges and brings forth future advancements. To enhance understanding in a rapidly evolving field, CHEST also features review articles, commentaries, and facilitates discussions on emerging controversies. We place great emphasis on scientific rigor, employing a rigorous peer review process, and ensuring all accepted content is published online within two weeks.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


