Long-Term Outcomes in Patients with ST-Elevation Myocardial Infarction: A Comparative Study of Direct Admissions versus Interhospital Transfers—Insights from a Single-Center Experience in the United Kingdom
{"title":"Long-Term Outcomes in Patients with ST-Elevation Myocardial Infarction: A Comparative Study of Direct Admissions versus Interhospital Transfers—Insights from a Single-Center Experience in the United Kingdom","authors":"Tarek Abdeldayem, Ashan Gunarathne","doi":"10.1155/2024/7112494","DOIUrl":null,"url":null,"abstract":"<div>\n <p><i>Background</i>. Primary percutaneous coronary intervention (PPCI) is the treatment of choice for patients with ST-elevation myocardial infarction (STEMI). Delayed reperfusion leads to increased morbidity and mortality. Secular trends in the impact of interhospital transfers (IT) on long-term mortality in the United Kingdom (UK) have not been previously investigated. We analyzed the impact of IT on 5-year mortality in STEMI patients admitted to a tertiary care center in the UK (East Midlands North). <i>Methods</i>. Data of STEMI patients admitted to Nottingham University Hospitals NHS Trust from 2011 to 2016 were acquired from the National Institute for Cardiovascular Outcomes Research dataset (NICOR) and then combined with local patient-level data and mortality data from National Statistics. The baseline characteristics and mortality data of the interhospital transfer (IT) group were compared to those of a gender and age-matched direct admission (DA) group. <i>Results</i>. Of the total cohort (<i>N</i> = 2386), 29.9% of patients were admitted to the PPCI center via the interhospital transfer (IT) route. Cardiovascular risk profiles in both DA and IT groups were comparable. Five-year Kaplan–Meier (KM) survival analysis revealed better survival in the direct admission group (83% vs. 77.3%; <i>p</i> ≤ 0.001). In multivariate analysis, increased mortality was associated with severe left ventricular impairment (HR 4.7, 95% CI 2.9–7.6), the presence of cardiogenic shock (HR 3.6 (2.7–4.8)), chronic kidney disease (HR 2.56 (1.4–4.5)), smoking (HR 1.45 (1.1–1.8)), male gender (HR 1.7 (1.4–2.01)), and diabetes (HR 1.4 (1.07–1.8)). The radial access and call-to-balloon time less than 120 minutes were also associated with lower mortality (HR 0.52 (0.43–0.63): HR 0.75 (0.61–0.92)). <i>Conclusion</i>. Despite advancements in communication, technology, patient education, transportation systems, and guidelines within the UK’s NHS over the last decade, the delays incurred by IT for STEMI patients remain substantial and are associated with a poor prognosis.</p>\n </div>","PeriodicalId":13782,"journal":{"name":"International Journal of Clinical Practice","volume":"2024 1","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2024-07-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/7112494","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Clinical Practice","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/2024/7112494","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
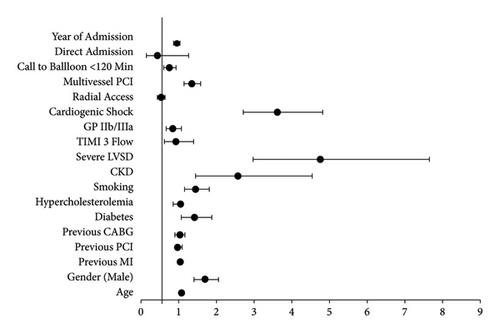
Background. Primary percutaneous coronary intervention (PPCI) is the treatment of choice for patients with ST-elevation myocardial infarction (STEMI). Delayed reperfusion leads to increased morbidity and mortality. Secular trends in the impact of interhospital transfers (IT) on long-term mortality in the United Kingdom (UK) have not been previously investigated. We analyzed the impact of IT on 5-year mortality in STEMI patients admitted to a tertiary care center in the UK (East Midlands North). Methods. Data of STEMI patients admitted to Nottingham University Hospitals NHS Trust from 2011 to 2016 were acquired from the National Institute for Cardiovascular Outcomes Research dataset (NICOR) and then combined with local patient-level data and mortality data from National Statistics. The baseline characteristics and mortality data of the interhospital transfer (IT) group were compared to those of a gender and age-matched direct admission (DA) group. Results. Of the total cohort (N = 2386), 29.9% of patients were admitted to the PPCI center via the interhospital transfer (IT) route. Cardiovascular risk profiles in both DA and IT groups were comparable. Five-year Kaplan–Meier (KM) survival analysis revealed better survival in the direct admission group (83% vs. 77.3%; p ≤ 0.001). In multivariate analysis, increased mortality was associated with severe left ventricular impairment (HR 4.7, 95% CI 2.9–7.6), the presence of cardiogenic shock (HR 3.6 (2.7–4.8)), chronic kidney disease (HR 2.56 (1.4–4.5)), smoking (HR 1.45 (1.1–1.8)), male gender (HR 1.7 (1.4–2.01)), and diabetes (HR 1.4 (1.07–1.8)). The radial access and call-to-balloon time less than 120 minutes were also associated with lower mortality (HR 0.52 (0.43–0.63): HR 0.75 (0.61–0.92)). Conclusion. Despite advancements in communication, technology, patient education, transportation systems, and guidelines within the UK’s NHS over the last decade, the delays incurred by IT for STEMI patients remain substantial and are associated with a poor prognosis.
期刊介绍:
IJCP is a general medical journal. IJCP gives special priority to work that has international appeal.
IJCP publishes:
Editorials. IJCP Editorials are commissioned. [Peer reviewed at the editor''s discretion]
Perspectives. Most IJCP Perspectives are commissioned. Example. [Peer reviewed at the editor''s discretion]
Study design and interpretation. Example. [Always peer reviewed]
Original data from clinical investigations. In particular: Primary research papers from RCTs, observational studies, epidemiological studies; pre-specified sub-analyses; pooled analyses. [Always peer reviewed]
Meta-analyses. [Always peer reviewed]
Systematic reviews. From October 2009, special priority will be given to systematic reviews. [Always peer reviewed]
Non-systematic/narrative reviews. From October 2009, reviews that are not systematic will be considered only if they include a discrete Methods section that must explicitly describe the authors'' approach. Special priority will, however, be given to systematic reviews. [Always peer reviewed]
''How to…'' papers. Example. [Always peer reviewed]
Consensus statements. [Always peer reviewed] Short reports. [Always peer reviewed]
Letters. [Peer reviewed at the editor''s discretion]
International scope
IJCP publishes work from investigators globally. Around 30% of IJCP articles list an author from the UK. Around 30% of IJCP articles list an author from the USA or Canada. Around 45% of IJCP articles list an author from a European country that is not the UK. Around 15% of articles published in IJCP list an author from a country in the Asia-Pacific region.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


