{"title":"Risk factors for sternal wound infection after median sternotomy: A nested case–control study and time-to-event analysis","authors":"Xiaolong Ma, Dongsheng Chen, Jianchao Liu, Wenqing Wang, Zekun Feng, Nan Cheng, Shuanglei Li, Shan Wang, Lihua Liu, Youbai Chen","doi":"10.1111/iwj.14965","DOIUrl":null,"url":null,"abstract":"<p>Although potential risk factors for sternal wound infection (SWI) have been extensively studied, the onset time of SWI and different risk factors for superficial and deep SWI were rarely reported. This nested case–control study aims to compare the onset time and contributors between superficial and deep SWI. Consecutive adult patients who underwent cardiac surgery through median sternotomy in a single center from January 2011 to January 2021 constituted the cohort. The case group was those who developed SWI as defined by CDC and controls were matched 6:1 per case. Kaplan–Meier analysis, LASSO and univariate and multivariate Cox regressions were performed. A simple nomogram was established for clinical prediction of the risk of SWI. The incidence of SWI was 1.1% (61 out of 5471) in our cohort. Totally 366 controls were matched to 61 cases. 26.2% (16 of 61) SWI cases were deep SWI. The median onset time of SWI was 35 days. DSWI had a longer latency than SSWI (median time 46 days vs. 32 days, <i>p</i> = 0.032). Kaplan–Meier analyses showed different time-to-SWI between patients with and without DM (<i>p</i> = 0.0011) or MI (<i>p</i> = 0.0019). Multivariate Cox regression showed that BMI (HR = 1.083, 95% CI: 1.012–1.116, <i>p</i> = 0.022), DM (HR = 2.041, 95% CI: 1.094–3.805, <i>p</i> = 0.025) and MI (HR = 2.332, 95% CI: 1.193–4.557, <i>p</i> = 0.013) were independent risk factors for SWI. Superficial SWI was only associated with BMI (HR = 1.089, 95% CI: 1.01–1.175, <i>p</i> = 0.027), while deep SWI was associated with DM (HR = 3.271, 95% CI: 1.036–10.325, <i>p</i> = 0.043) and surgery time (HR = 1.004, 95% CI: 1.001–1.008, <i>p</i> = 0.027). The nomogram for SWI prediction had an AUC of 0.67, good fitness and clinical effectiveness as shown by the calibration curve and decision curve analyses. BMI, DM and MI were independent risk factors for SWI. DSWI had a longer latency and different risk factors compared to SSWI. The nomogram showed a fair performance and good effectiveness for the clinical prediction of SWI.</p>","PeriodicalId":14451,"journal":{"name":"International Wound Journal","volume":null,"pages":null},"PeriodicalIF":2.6000,"publicationDate":"2024-07-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11240533/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Wound Journal","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/iwj.14965","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
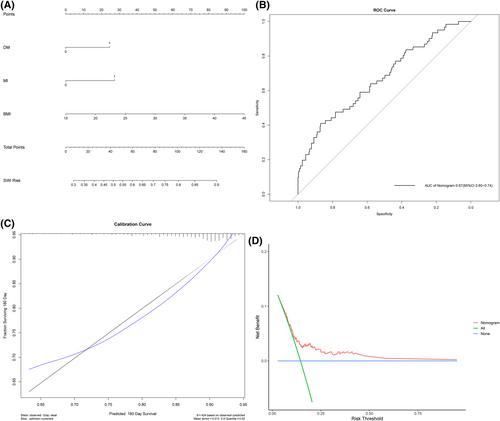
Although potential risk factors for sternal wound infection (SWI) have been extensively studied, the onset time of SWI and different risk factors for superficial and deep SWI were rarely reported. This nested case–control study aims to compare the onset time and contributors between superficial and deep SWI. Consecutive adult patients who underwent cardiac surgery through median sternotomy in a single center from January 2011 to January 2021 constituted the cohort. The case group was those who developed SWI as defined by CDC and controls were matched 6:1 per case. Kaplan–Meier analysis, LASSO and univariate and multivariate Cox regressions were performed. A simple nomogram was established for clinical prediction of the risk of SWI. The incidence of SWI was 1.1% (61 out of 5471) in our cohort. Totally 366 controls were matched to 61 cases. 26.2% (16 of 61) SWI cases were deep SWI. The median onset time of SWI was 35 days. DSWI had a longer latency than SSWI (median time 46 days vs. 32 days, p = 0.032). Kaplan–Meier analyses showed different time-to-SWI between patients with and without DM (p = 0.0011) or MI (p = 0.0019). Multivariate Cox regression showed that BMI (HR = 1.083, 95% CI: 1.012–1.116, p = 0.022), DM (HR = 2.041, 95% CI: 1.094–3.805, p = 0.025) and MI (HR = 2.332, 95% CI: 1.193–4.557, p = 0.013) were independent risk factors for SWI. Superficial SWI was only associated with BMI (HR = 1.089, 95% CI: 1.01–1.175, p = 0.027), while deep SWI was associated with DM (HR = 3.271, 95% CI: 1.036–10.325, p = 0.043) and surgery time (HR = 1.004, 95% CI: 1.001–1.008, p = 0.027). The nomogram for SWI prediction had an AUC of 0.67, good fitness and clinical effectiveness as shown by the calibration curve and decision curve analyses. BMI, DM and MI were independent risk factors for SWI. DSWI had a longer latency and different risk factors compared to SSWI. The nomogram showed a fair performance and good effectiveness for the clinical prediction of SWI.
期刊介绍:
The Editors welcome papers on all aspects of prevention and treatment of wounds and associated conditions in the fields of surgery, dermatology, oncology, nursing, radiotherapy, physical therapy, occupational therapy and podiatry. The Journal accepts papers in the following categories:
- Research papers
- Review articles
- Clinical studies
- Letters
- News and Views: international perspectives, education initiatives, guidelines and different activities of groups and societies.
Calendar of events
The Editors are supported by a board of international experts and a panel of reviewers across a range of disciplines and specialties which ensures only the most current and relevant research is published.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


