Emily E Zona, Mina L Gibes, Asha S Jain, Jeannina A Smith, Jacqueline M Garonzik-Wang, Didier A Mandelbrot, Sandesh Parajuli
{"title":"Long-term follow-up of kidney transplant recipients admitted to a tertiary care transplant center with SARS-CoV-2.","authors":"Emily E Zona, Mina L Gibes, Asha S Jain, Jeannina A Smith, Jacqueline M Garonzik-Wang, Didier A Mandelbrot, Sandesh Parajuli","doi":"10.5501/wjv.v13.i2.95273","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Kidney transplant recipients (KTR) are at risk of severe coronavirus disease 2019 (COVID-19) disease and mortality after severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. We predicted that hospitalization for COVID-19 and subsequent admission to the intensive care unit (ICU) would yield worse outcomes in KTRs.</p><p><strong>Aim: </strong>To investigate outcomes among KTRs hospitalized at our high-volume transplant center either on the general hospital floor or the ICU.</p><p><strong>Methods: </strong>We retrospectively describe all adult KTRs who were hospitalized at our center with their first SARS-CoV-2 infection between 04/2020 and 04/2022 and had at least 12 months follow-up (unless they experienced graft failure or death). The cohort was stratified by ICU admission. Outcomes of interest included risk factors for ICU admission and mortality, length of stay (LOS), respiratory symptoms at admission, all-cause graft failure at the last follow-up, and death related to COVID-19.</p><p><strong>Results: </strong>96 KTRs were hospitalized for SARS-COV-2 infection. 21 (22%) required ICU admission. The ICU group had longer hospital LOS (21.8 <i>vs</i> 8.6 days, <i>P</i> < 0.001) and were more likely to experience graft failure (81% <i>vs</i> 31%, <i>P</i> < 0.001). Of those admitted to the ICU, 76% had death at last-follow up, and 71% had death related to COVID-19. Risk factors for ICU admission included male sex (aHR: 3.11, 95%CI: 1.04-9.34; <i>P</i> = 0.04). Risk factors for all-cause mortality and COVID-19-related mortality included ICU admission and advanced age at SARS-CoV-2 diagnosis. Mortality was highest within a month of COVID-19 diagnosis, with the ICU group having increased risk of all-cause (aHR: 11.2, 95%CI: 5.11-24.5; <i>P</i> < 0.001) and COVID-19-related mortality (aHR: 27.2, 95%CI: 8.69-84.9; <i>P</i> < 0.001).</p><p><strong>Conclusion: </strong>ICU admission conferred an increased risk of mortality, graft failure, and longer LOS. One-fifth of those hospitalized died of COVID-19, reflecting the impact of COVID-19-related morbidity and mortality among KTRs.</p>","PeriodicalId":61903,"journal":{"name":"世界病毒学杂志(英文版)","volume":"13 2","pages":"95273"},"PeriodicalIF":0.0000,"publicationDate":"2024-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11229845/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界病毒学杂志(英文版)","FirstCategoryId":"1089","ListUrlMain":"https://doi.org/10.5501/wjv.v13.i2.95273","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Kidney transplant recipients (KTR) are at risk of severe coronavirus disease 2019 (COVID-19) disease and mortality after severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. We predicted that hospitalization for COVID-19 and subsequent admission to the intensive care unit (ICU) would yield worse outcomes in KTRs.
Aim: To investigate outcomes among KTRs hospitalized at our high-volume transplant center either on the general hospital floor or the ICU.
Methods: We retrospectively describe all adult KTRs who were hospitalized at our center with their first SARS-CoV-2 infection between 04/2020 and 04/2022 and had at least 12 months follow-up (unless they experienced graft failure or death). The cohort was stratified by ICU admission. Outcomes of interest included risk factors for ICU admission and mortality, length of stay (LOS), respiratory symptoms at admission, all-cause graft failure at the last follow-up, and death related to COVID-19.
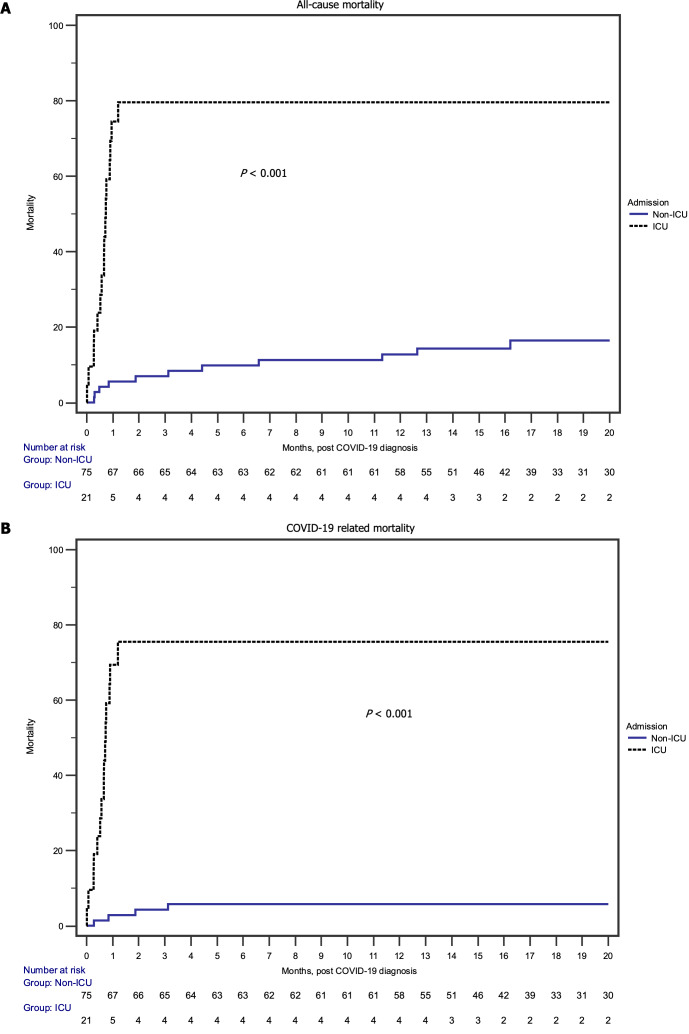
Results: 96 KTRs were hospitalized for SARS-COV-2 infection. 21 (22%) required ICU admission. The ICU group had longer hospital LOS (21.8 vs 8.6 days, P < 0.001) and were more likely to experience graft failure (81% vs 31%, P < 0.001). Of those admitted to the ICU, 76% had death at last-follow up, and 71% had death related to COVID-19. Risk factors for ICU admission included male sex (aHR: 3.11, 95%CI: 1.04-9.34; P = 0.04). Risk factors for all-cause mortality and COVID-19-related mortality included ICU admission and advanced age at SARS-CoV-2 diagnosis. Mortality was highest within a month of COVID-19 diagnosis, with the ICU group having increased risk of all-cause (aHR: 11.2, 95%CI: 5.11-24.5; P < 0.001) and COVID-19-related mortality (aHR: 27.2, 95%CI: 8.69-84.9; P < 0.001).
Conclusion: ICU admission conferred an increased risk of mortality, graft failure, and longer LOS. One-fifth of those hospitalized died of COVID-19, reflecting the impact of COVID-19-related morbidity and mortality among KTRs.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


