Long-term posttransplant survival outcome following bridging locoregional therapy in hepatocellular carcinoma patients: A systematic review and meta-analysis
{"title":"Long-term posttransplant survival outcome following bridging locoregional therapy in hepatocellular carcinoma patients: A systematic review and meta-analysis","authors":"Alan Chuncharunee, Songporn Oranratnachai, Lancharat Chuncharunee, Pongphob Intaraprasong, Ammarin Thakkinstian, Abhasnee Sobhonslidsuk","doi":"10.1002/jgh3.13111","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aim</h3>\n \n <p>Liver transplantation (LT) is essential due to its curative efficacy, but liver-graft shortages have limited its widespread application. Bridging locoregional therapy (LRT) before LT has been performed to prevent tumor progression, and a recent literature review revealed that it is associated with a nonsignificant trend toward better survival outcomes. However, much more information on bridging therapy has become available since then. This meta-analysis aimed to compare the posttransplant survival and HCC recurrence between patients with and without pretransplant bridging LRT.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Studies were identified in MEDLINE, SCOPUS, and the Cochrane Library. Two independent researchers screened titles and full articles, extracted relevant data, and conducted a parametric survival analysis.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Out of 4794 studies, 18 cohort studies were eligible. The 1-, 3-, and 5-year overall survival (OS) rates were 93.1%, 85.0%, and 79.1% for those in the bridging LRT group, while they were 91.8%, 81.1%, and 75.5% for those who did not receive LRT, respectively. There were no differences in overall survival between these groups (HR 0.90; 0.78–1.05, P = 0.17). Interestingly, we discovered that bridging therapy helped prolong survival significantly in a high-risk population with a long waiting time (HR 0.76; 0.60–0.96, P = 0.02). Unfortunately, bridging LRT did not improve disease-free survival (HR 0.98; 0.86–1.11, P = 0.70).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>The results indicate that bridging LRT does not generally change post-LT outcomes. However, bridging LRT can significantly improve survival in patients with a long waiting time for LT.</p>\n </section>\n </div>","PeriodicalId":45861,"journal":{"name":"JGH Open","volume":"8 7","pages":""},"PeriodicalIF":1.7000,"publicationDate":"2024-07-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11228543/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JGH Open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jgh3.13111","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Aim
Liver transplantation (LT) is essential due to its curative efficacy, but liver-graft shortages have limited its widespread application. Bridging locoregional therapy (LRT) before LT has been performed to prevent tumor progression, and a recent literature review revealed that it is associated with a nonsignificant trend toward better survival outcomes. However, much more information on bridging therapy has become available since then. This meta-analysis aimed to compare the posttransplant survival and HCC recurrence between patients with and without pretransplant bridging LRT.
Methods
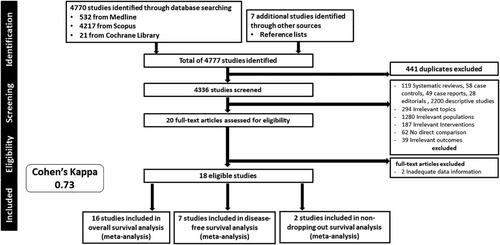
Studies were identified in MEDLINE, SCOPUS, and the Cochrane Library. Two independent researchers screened titles and full articles, extracted relevant data, and conducted a parametric survival analysis.
Results
Out of 4794 studies, 18 cohort studies were eligible. The 1-, 3-, and 5-year overall survival (OS) rates were 93.1%, 85.0%, and 79.1% for those in the bridging LRT group, while they were 91.8%, 81.1%, and 75.5% for those who did not receive LRT, respectively. There were no differences in overall survival between these groups (HR 0.90; 0.78–1.05, P = 0.17). Interestingly, we discovered that bridging therapy helped prolong survival significantly in a high-risk population with a long waiting time (HR 0.76; 0.60–0.96, P = 0.02). Unfortunately, bridging LRT did not improve disease-free survival (HR 0.98; 0.86–1.11, P = 0.70).
Conclusions
The results indicate that bridging LRT does not generally change post-LT outcomes. However, bridging LRT can significantly improve survival in patients with a long waiting time for LT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


