Blood pressure during long-term cilostazol-based dual antiplatelet therapy after stroke: a post hoc analysis of the CSPS.com trial
IF 4.3
2区 医学
Q1 PERIPHERAL VASCULAR DISEASE
引用次数: 0
Abstract
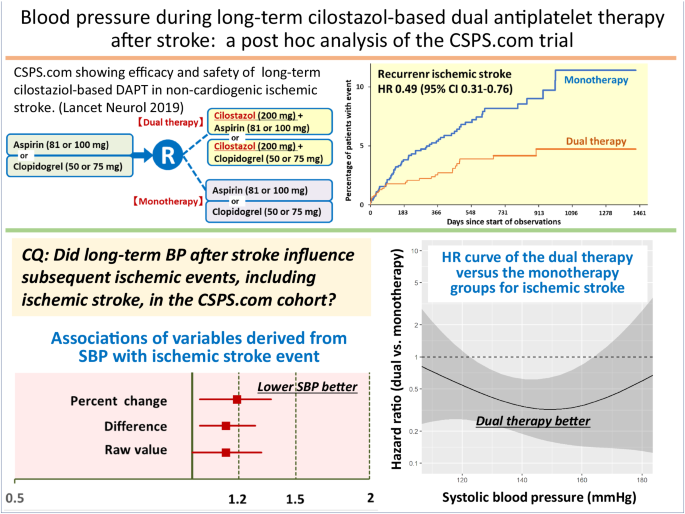
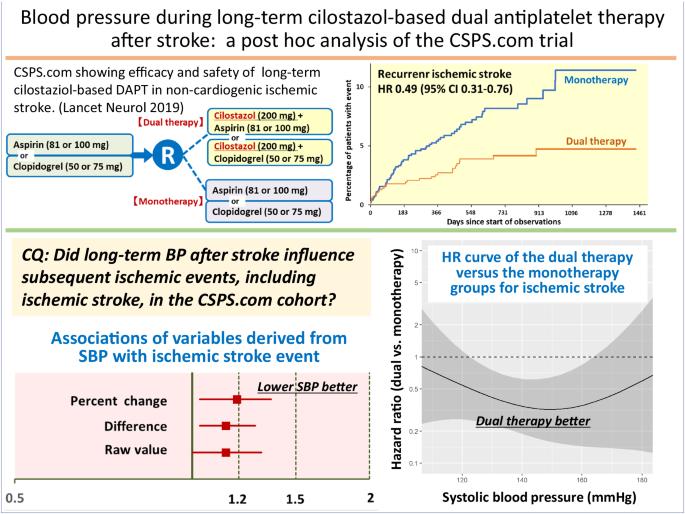
We determined the associations of follow-up blood pressure (BP) after stroke as a time-dependent covariate with the risk of subsequent ischemic stroke, as well as those of BP levels with the difference in the impact of long-term clopidogrel or aspirin monotherapy versus additional cilostazol medication on secondary stroke prevention. In a sub-analysis of a randomized controlled trial (CSPS.com), patients between 8 and 180 days after stroke onset were randomly assigned to receive aspirin or clopidogrel alone, or a combination of cilostazol with aspirin or clopidogrel. The percent changes, differences, and raw values of follow-up BP were examined. The primary efficacy outcome was the first recurrence of ischemic stroke. In a total of 1657 patients (69.5 ± 9.3 years, female 29.1%) with median 1.5-year follow-up, ischemic stroke recurred in 74 patients. The adjusted hazard ratio for ischemic stroke of a 10% systolic BP (SBP) increase from baseline was 1.19 (95% CI 1.03–1.36), that of a 10 mmHg SBP increase was 1.14 (1.03–1.28), and that of SBP as the raw value with the baseline SBP as a fixed (time-independent) covariate was 1.14 (1.00–1.31). Such significant associations were not observed in diastolic BP-derived variables. The estimated adjusted hazard ratio curves for the outcome showed the benefit of dual therapy over a wide SBP range between ≈120 and ≈165 mmHg uniformly. Lower long-term SBP levels after ischemic stroke were associated with a lower risk of subsequent ischemic events. The efficacy of dual antiplatelet therapy including cilostazol for secondary stroke prevention was evident over a wide SBP range.
中风后基于西洛他唑的长期双联抗血小板疗法期间的血压:CSPS.com 试验的事后分析。
我们确定了中风后随访血压(BP)作为随时间变化的协变量与后续缺血性中风风险的关系,以及血压水平与长期氯吡格雷或阿司匹林单药治疗与额外服用西洛他唑对中风二级预防的影响差异的关系。在一项随机对照试验(CSPS.com)的子分析中,中风发作后 8 到 180 天的患者被随机分配到单独接受阿司匹林或氯吡格雷治疗,或西洛他唑与阿司匹林或氯吡格雷联合治疗。对随访血压的百分比变化、差异和原始值进行了研究。主要疗效结果是缺血性脑卒中首次复发。在中位随访 1.5 年的 1657 例患者(69.5 ± 9.3 岁,女性占 29.1%)中,有 74 例患者再次发生缺血性中风。收缩压(SBP)比基线升高 10%,缺血性脑卒中的调整危险比为 1.19(95% CI 1.03-1.36),SBP 升高 10 mmHg,缺血性脑卒中的调整危险比为 1.14(1.03-1.28),SBP 为原始值,基线 SBP 为固定(与时间无关)协变量,缺血性脑卒中的调整危险比为 1.14(1.00-1.31)。在舒张压衍生变量中没有观察到这种明显的关联。结果的估计调整危险比曲线显示,在SBP≈120和≈165 mmHg之间的宽范围内,双重疗法的益处是一致的。缺血性脑卒中后长期SBP水平较低与随后发生缺血性事件的风险较低有关。包括西洛他唑在内的双重抗血小板疗法对中风二级预防的疗效在较宽的 SBP 范围内都很明显。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Hypertension Research
医学-外周血管病
CiteScore
7.40
自引率
16.70%
发文量
249
审稿时长
3-8 weeks
期刊介绍:
Hypertension Research is the official publication of the Japanese Society of Hypertension. The journal publishes papers reporting original clinical and experimental research that contribute to the advancement of knowledge in the field of hypertension and related cardiovascular diseases. The journal publishes Review Articles, Articles, Correspondence and Comments.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


