Anti-PD-1/L1 antibody plus anti-VEGF antibody vs. plus VEGFR-targeted TKI as first-line therapy for unresectable hepatocellular carcinoma: a network meta-analysis.
{"title":"Anti-PD-1/L1 antibody plus anti-VEGF antibody <i>vs.</i> plus VEGFR-targeted TKI as first-line therapy for unresectable hepatocellular carcinoma: a network meta-analysis.","authors":"Yiwen Zhou, Jingjing Li, Jieer Ying","doi":"10.37349/etat.2024.00236","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This article is based on our previous research, which was presented at the 2023 ASCO Annual Meeting I and published in <i>Journal of Clinical Oncology</i> as Conference Abstract (<i>JCO</i>. 2023;41:e16148. doi: 10.1200/JCO.2023.41.16_suppl.e16148). Both anti-programmed death 1/ligand-1 (PD-1/L1) antibody + anti-vascular endothelial growth factor (VEGF) antibody (A + A) and anti-PD-1/L1 antibody + VEGF receptor (VEGFR)-targeted tyrosine kinase inhibitor (A + T) are effective first-line therapies for unresectable hepatocellular carcinoma. However, there lacks evidence from head-to-head comparisons between these two treatments. We conducted a network meta-analysis on the efficacy and safety of them.</p><p><strong>Methods: </strong>After a rigorous literature research, 6 phase III trials were identified for the final analysis, including IMbrave150, ORIENT-32, COSMIC-312, CARES-310, LEAP-002, and REFLECT. The experiments were classified into three groups: A + A, A + T, and intermediate reference group. The primary endpoint was overall survival (OS), and secondary endpoints included progression-free survival (PFS), objective response rate (ORR), and incidence of treatment-related adverse events (TRAEs). Hazard ratio (HR) with 95% confidence intervals (CI) for OS and PFS, odds ratio (OR) for ORR, and relative risk (RR) for all grade and grade ≥3 TRAEs were calculated. Under Bayesian framework, the meta-analysis was conducted using sorafenib as intermediate reference.</p><p><strong>Results: </strong>With the rank probability of 96%, A + A showed the greatest reduction in the risk of death, without significant difference from A + T (HR: 0.82, 95% CI: 0.65-1.04). A + T showed the greatest effect in prolonging PFS and improving ORR with the rank probability of 77%, but there were no statistical differences with A + A. A + A was safer than A + T in terms of all grade of TRAEs (RR: 0.91, 95% CI: 0.82-1.00) and particularly in those grade ≥3 (RR: 0.65, 95% CI: 0.54-0.77).</p><p><strong>Conclusions: </strong>A + A had the greatest probability of delivering the longest OS, while A + T was correlated with larger PFS benefits at the cost of a lower safety rate.</p>","PeriodicalId":73002,"journal":{"name":"Exploration of targeted anti-tumor therapy","volume":"5 3","pages":"568-580"},"PeriodicalIF":0.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11220314/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Exploration of targeted anti-tumor therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.37349/etat.2024.00236","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/17 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This article is based on our previous research, which was presented at the 2023 ASCO Annual Meeting I and published in Journal of Clinical Oncology as Conference Abstract (JCO. 2023;41:e16148. doi: 10.1200/JCO.2023.41.16_suppl.e16148). Both anti-programmed death 1/ligand-1 (PD-1/L1) antibody + anti-vascular endothelial growth factor (VEGF) antibody (A + A) and anti-PD-1/L1 antibody + VEGF receptor (VEGFR)-targeted tyrosine kinase inhibitor (A + T) are effective first-line therapies for unresectable hepatocellular carcinoma. However, there lacks evidence from head-to-head comparisons between these two treatments. We conducted a network meta-analysis on the efficacy and safety of them.
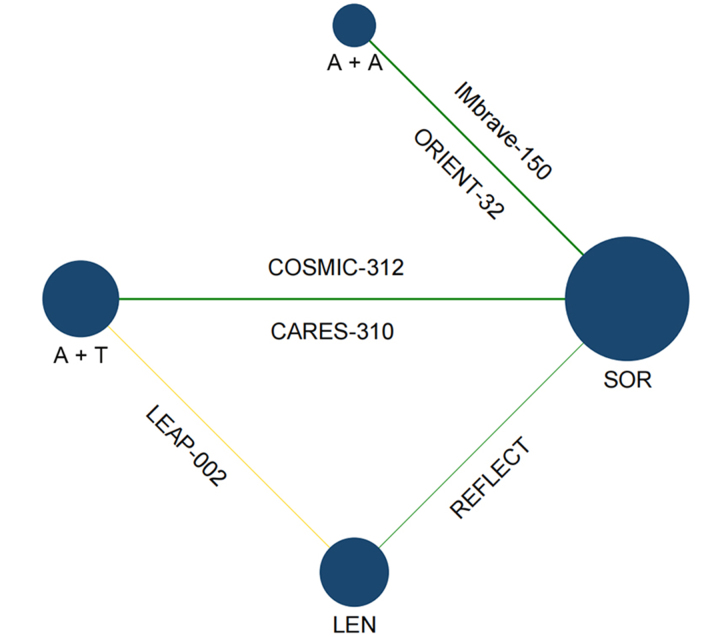
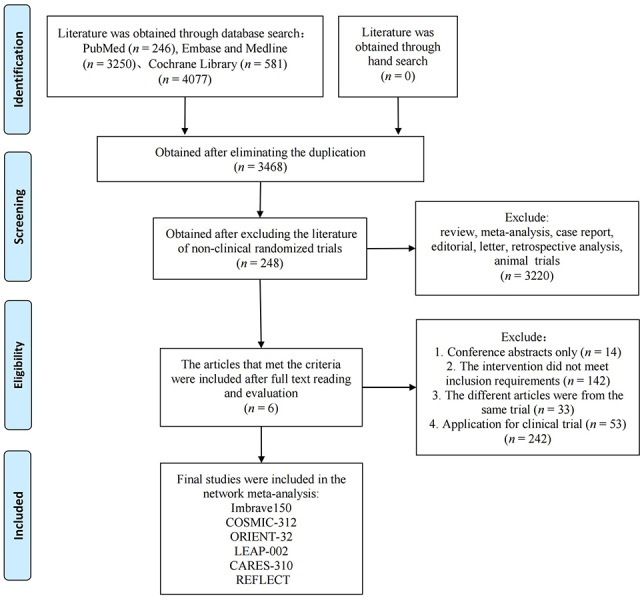
Methods: After a rigorous literature research, 6 phase III trials were identified for the final analysis, including IMbrave150, ORIENT-32, COSMIC-312, CARES-310, LEAP-002, and REFLECT. The experiments were classified into three groups: A + A, A + T, and intermediate reference group. The primary endpoint was overall survival (OS), and secondary endpoints included progression-free survival (PFS), objective response rate (ORR), and incidence of treatment-related adverse events (TRAEs). Hazard ratio (HR) with 95% confidence intervals (CI) for OS and PFS, odds ratio (OR) for ORR, and relative risk (RR) for all grade and grade ≥3 TRAEs were calculated. Under Bayesian framework, the meta-analysis was conducted using sorafenib as intermediate reference.
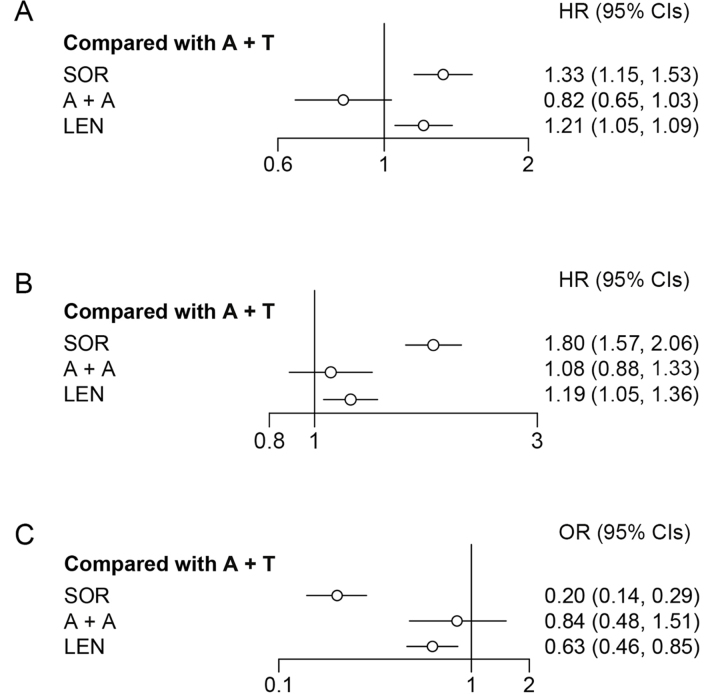
Results: With the rank probability of 96%, A + A showed the greatest reduction in the risk of death, without significant difference from A + T (HR: 0.82, 95% CI: 0.65-1.04). A + T showed the greatest effect in prolonging PFS and improving ORR with the rank probability of 77%, but there were no statistical differences with A + A. A + A was safer than A + T in terms of all grade of TRAEs (RR: 0.91, 95% CI: 0.82-1.00) and particularly in those grade ≥3 (RR: 0.65, 95% CI: 0.54-0.77).
Conclusions: A + A had the greatest probability of delivering the longest OS, while A + T was correlated with larger PFS benefits at the cost of a lower safety rate.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


