{"title":"Lack of detection of aluminium-reactive T-lymphocytes in patients with SCIT-induced granulomas","authors":"Stine Skovbo Hoffmann, Jesper Elberling, Jeanne Duus Johansen, Lars Heede Blom","doi":"10.1002/clt2.12378","DOIUrl":null,"url":null,"abstract":"<p>Aluminium contact allergy is mainly seen in children with itching vaccination granulomas following immunization with aluminium-adsorbed vaccines, but may also occur in adults following allergen-specific subcutaneous immunotherapy, SCIT, as these vaccines too are aluminium-adsorbed.<span><sup>1</sup></span> Traditional method of determining sensitization to aluminium is patch testing, an in vivo skin test considered the gold standard for detecting contact allergy.<span><sup>2</sup></span> Still, it has the disadvantage of only detecting the allergic response in the skin, and not systemic reactions. In adults there is a great risk of false-negative patch test results even though new recommendations on a higher aluminium concentration, rising from 2% to 10% aluminium chloride hexahydrate (AlCl<sub>3</sub>H<sub>2</sub>O<sub>6</sub>), has been implemented.<span><sup>3</sup></span></p><p>An alternative to patch testing is the blood in vitro lymphocyte proliferation test (LPT), also known as the lymphocyte transformation test (LTT), which we investigated using a well-established LPT protocol. This has previously been shown to detect and characterize metal-specific cells and was used to detect circulating aluminium-specific proliferation. The LPT test is based on a single blood sample and has mostly been used to detect drug hypersensitivity. Still, its role in detecting metal allergy is expanding,<span><sup>4</sup></span> with recent studies suggesting using the test as a supplement to the patch test when only a few allergens are to be investigated.<span><sup>5</sup></span> Our study aimed to determine the diagnostic performance of LPT in adults with SCIT-induced vaccination granulomas, and to evaluate the association between LPT and patch test reactions.</p><p>We included six participants with SCIT-induced granulomas and 10 healthy controls. Inclusion of patients was limited by the small number of SCIT-recipients referred to our department.</p><p>Characteristics of the participants with SCIT-induced granulomas are shown in Table 1. All granulomas were long-lasting, and except for one participant with 2 granulomas, all had 3 or more palpable and itching granulomas, mainly on the upper arms but also on the flanks. The control group were matched for age and sex, and did not undergo patch testing, but had no history of post-vaccination granulomas, contact dermatitis, contact allergy, or other skin diseases, had never received SCIT and not been vaccinated with an aluminium-adsorbed vaccine within the last year.</p><p>Participants with granulomas were all patch tested with AlCl<sub>3</sub>H<sub>2</sub>O<sub>6</sub> 2% (before 2021) or 10% mixed in petrolatum and applied under Finn chambers, an aluminium Finn chamber and an empty plastic chamber as control (8 mm; Smartpractice, Phoenix, AZ, USA), all applied on the upper back and secured with Scanpor<sup>®</sup> tape (Norgesplaster, Vennesla, Norway). Application time was 2 days, and patch test reactions were scored on day 2, 3–4 and 7.</p><p>Two participants with granulomas had a positive patch test reaction to aluminium AlCl<sub>3</sub>H<sub>2</sub>O<sub>6</sub> either 2% or 10% pet, and none had a positive reaction to the metallic aluminium disc.</p><p>Following blood sampling, peripheral blood mononuclear cells (PBMC) were purified by gradient centrifugation from the blood of participants with SCIT-induced granulomas and healthy subjects. After PBMC purification, the cells was stained with carboxyfluorescein diacetate succinimidyl ester (CFSE) as described before.<span><sup>5</sup></span> Specific proliferation of PBMCs was seen after stimulation with the positive control antigen, tetanus, in participants with SCIT-induced granulomas and healthy subjects (Figure 1A,B), indicating responsive PBMCs. As recommended when setting up an LTT assay,<span><sup>6</sup></span> the CFSE-labeled PBMCs were stimulated with the highest three non-toxic concentrations (1.95, 7.8 and 31.3 μg/mL) of AlCl<sub>3</sub>H<sub>2</sub>O<sub>6</sub> (Sigma, Missouri, USA) for 7 days. On day seven of culture, the PBMCs were stained with subtype and tissue-associated marker antibodies and analysed by flow cytometry. Further description of the method is available in Supplementary Appendix.</p><p>In stimulation with three non-toxic concentrations of aluminium, no differences were found comparing the stimulation index (SI) of proliferating (CFSE<sup>low</sup>) cells and memory (CD45RO+) T cells in healthy subjects and participants with SCIT-induced granulomas (Figure 1A,B). Aluminium-induced proliferation was only detected in the T helper (Th) cells in two healthy subjects and one participant with SCIT-induced granulomas (Figure 1C). Only one (participant 6) of the six participants with SCIT-induced granulomas had a specific proliferation of Th cells expressing the skin signature marker cutaneous lymphocyte-associated antigen (CLA) (Figure 1D), although patch testing was negative.</p><p>The findings in this preliminary study indicate that there might be few or no circulating aluminium-reactive cells in adults, despite continuing itch from the granulomas. Both the patch test and the LPT test may have low sensitivity for detecting aluminium contact allergy in adults.<span><sup>4</sup></span> Other possible explanations for the negative test results are that the T cell-dependent inflammation in the granulomas is not caused by aluminium, as granulomas have various histopathological findings,<span><sup>7</sup></span> or perhaps the aluminium allergy has diminished due to the time interval between induction/elicitation and testing as reported in other studies.<span><sup>8</sup></span> Moreover, the lack of specific proliferation in the LTT system could also be due to the formulation of aluminium or lagging formation of aluminium-protein hapten complexes in vitro.</p><p>Since oral intake of aluminium may generate a systemic response with cutaneous eruptions in children with vaccination granulomas,<span><sup>9</sup></span> a study on the lymphocyte reactivity characterizing the possibility of systemic reactions in these children would be of great interest.</p><p><b>Stine Skovbo Hoffmann</b>: Data curation; investigation; writing – original draft; writing – review & editing. <b>Jesper Elberling</b>: Conceptualization; supervision; writing – review & editing. <b>Jeanne Duus Johansen</b>: Conceptualization; methodology; supervision; writing – review & editing. <b>Lars Heede Blom</b>: Conceptualization; formal analysis; software; writing – review & editing.</p><p>None.</p>","PeriodicalId":10334,"journal":{"name":"Clinical and Translational Allergy","volume":"14 7","pages":""},"PeriodicalIF":4.6000,"publicationDate":"2024-07-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11217595/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clt2.12378","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Aluminium contact allergy is mainly seen in children with itching vaccination granulomas following immunization with aluminium-adsorbed vaccines, but may also occur in adults following allergen-specific subcutaneous immunotherapy, SCIT, as these vaccines too are aluminium-adsorbed.1 Traditional method of determining sensitization to aluminium is patch testing, an in vivo skin test considered the gold standard for detecting contact allergy.2 Still, it has the disadvantage of only detecting the allergic response in the skin, and not systemic reactions. In adults there is a great risk of false-negative patch test results even though new recommendations on a higher aluminium concentration, rising from 2% to 10% aluminium chloride hexahydrate (AlCl3H2O6), has been implemented.3
An alternative to patch testing is the blood in vitro lymphocyte proliferation test (LPT), also known as the lymphocyte transformation test (LTT), which we investigated using a well-established LPT protocol. This has previously been shown to detect and characterize metal-specific cells and was used to detect circulating aluminium-specific proliferation. The LPT test is based on a single blood sample and has mostly been used to detect drug hypersensitivity. Still, its role in detecting metal allergy is expanding,4 with recent studies suggesting using the test as a supplement to the patch test when only a few allergens are to be investigated.5 Our study aimed to determine the diagnostic performance of LPT in adults with SCIT-induced vaccination granulomas, and to evaluate the association between LPT and patch test reactions.
We included six participants with SCIT-induced granulomas and 10 healthy controls. Inclusion of patients was limited by the small number of SCIT-recipients referred to our department.
Characteristics of the participants with SCIT-induced granulomas are shown in Table 1. All granulomas were long-lasting, and except for one participant with 2 granulomas, all had 3 or more palpable and itching granulomas, mainly on the upper arms but also on the flanks. The control group were matched for age and sex, and did not undergo patch testing, but had no history of post-vaccination granulomas, contact dermatitis, contact allergy, or other skin diseases, had never received SCIT and not been vaccinated with an aluminium-adsorbed vaccine within the last year.
Participants with granulomas were all patch tested with AlCl3H2O6 2% (before 2021) or 10% mixed in petrolatum and applied under Finn chambers, an aluminium Finn chamber and an empty plastic chamber as control (8 mm; Smartpractice, Phoenix, AZ, USA), all applied on the upper back and secured with Scanpor® tape (Norgesplaster, Vennesla, Norway). Application time was 2 days, and patch test reactions were scored on day 2, 3–4 and 7.
Two participants with granulomas had a positive patch test reaction to aluminium AlCl3H2O6 either 2% or 10% pet, and none had a positive reaction to the metallic aluminium disc.
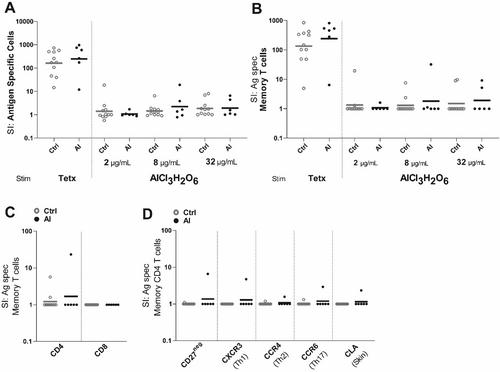
Following blood sampling, peripheral blood mononuclear cells (PBMC) were purified by gradient centrifugation from the blood of participants with SCIT-induced granulomas and healthy subjects. After PBMC purification, the cells was stained with carboxyfluorescein diacetate succinimidyl ester (CFSE) as described before.5 Specific proliferation of PBMCs was seen after stimulation with the positive control antigen, tetanus, in participants with SCIT-induced granulomas and healthy subjects (Figure 1A,B), indicating responsive PBMCs. As recommended when setting up an LTT assay,6 the CFSE-labeled PBMCs were stimulated with the highest three non-toxic concentrations (1.95, 7.8 and 31.3 μg/mL) of AlCl3H2O6 (Sigma, Missouri, USA) for 7 days. On day seven of culture, the PBMCs were stained with subtype and tissue-associated marker antibodies and analysed by flow cytometry. Further description of the method is available in Supplementary Appendix.
In stimulation with three non-toxic concentrations of aluminium, no differences were found comparing the stimulation index (SI) of proliferating (CFSElow) cells and memory (CD45RO+) T cells in healthy subjects and participants with SCIT-induced granulomas (Figure 1A,B). Aluminium-induced proliferation was only detected in the T helper (Th) cells in two healthy subjects and one participant with SCIT-induced granulomas (Figure 1C). Only one (participant 6) of the six participants with SCIT-induced granulomas had a specific proliferation of Th cells expressing the skin signature marker cutaneous lymphocyte-associated antigen (CLA) (Figure 1D), although patch testing was negative.
The findings in this preliminary study indicate that there might be few or no circulating aluminium-reactive cells in adults, despite continuing itch from the granulomas. Both the patch test and the LPT test may have low sensitivity for detecting aluminium contact allergy in adults.4 Other possible explanations for the negative test results are that the T cell-dependent inflammation in the granulomas is not caused by aluminium, as granulomas have various histopathological findings,7 or perhaps the aluminium allergy has diminished due to the time interval between induction/elicitation and testing as reported in other studies.8 Moreover, the lack of specific proliferation in the LTT system could also be due to the formulation of aluminium or lagging formation of aluminium-protein hapten complexes in vitro.
Since oral intake of aluminium may generate a systemic response with cutaneous eruptions in children with vaccination granulomas,9 a study on the lymphocyte reactivity characterizing the possibility of systemic reactions in these children would be of great interest.
期刊介绍:
Clinical and Translational Allergy, one of several journals in the portfolio of the European Academy of Allergy and Clinical Immunology, provides a platform for the dissemination of allergy research and reviews, as well as EAACI position papers, task force reports and guidelines, amongst an international scientific audience.
Clinical and Translational Allergy accepts clinical and translational research in the following areas and other related topics: asthma, rhinitis, rhinosinusitis, drug hypersensitivity, allergic conjunctivitis, allergic skin diseases, atopic eczema, urticaria, angioedema, venom hypersensitivity, anaphylaxis, food allergy, immunotherapy, immune modulators and biologics, animal models of allergic disease, immune mechanisms, or any other topic related to allergic disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


