{"title":"Effectiveness of direct needle puncture for complete hepaticojejunostomy anastomotic stricture after pancreaticoduodenectomy (with video)","authors":"Koichi Soga, Fuki Hayakawa, Takeshi Fujiwara, Yoshinori Gyotoku, Yumi Kusano, Ikuhiro Kobori, Masaya Tamano","doi":"10.1002/deo2.396","DOIUrl":null,"url":null,"abstract":"<p>A 79-year-old Japanese woman, who had undergone pancreaticoduodenectomy 6 months prior to presentation owing to pancreatic cancer, complained of jaundice with high fever. Computed tomography revealed proximal bile duct dilatation with complete hepaticojejunostomy anastomotic stricture (HJAS). We performed a single-balloon endoscopy for biliary drainage. The presence of a scar-like feature surrounding the anastomosis was identified as the HJAS. White-light imaging during single-balloon endoscopy revealed that the HJAS contained a milky whitish area (MWA), suggesting that a membranous and fibrosis layer affected continuous inflammation around the center of the anastomosis (within a scar-like feature). Endoscopic dilatation was performed using an endoscopic injection needle, with the MWA used as an indicator. A 23-gauge endoscopic injection needle was used to penetrate the center of the blind lumen within the MWA, and a pinhole was created in the stricture. After confirming the position of the proximal bile duct using a contrast medium with the needle, an endoscopic guidewire with a cannula was inserted into the pinhole. A through-the-scope sequential balloon dilator was used to dilate the stricture, and a plastic stent was inserted into the proximal bile duct. This endoscopic intervention led to positive outcomes. In cases of complete HJAS occlusion, an endoscopic approach to the bile duct is difficult because the anastomotic opening of the HJAS is not visible. Thus, puncturing within the MWA, which can be used as a scar-like landmark within a complete membranous HJAS, is considered a useful endoscopic strategy.</p>","PeriodicalId":93973,"journal":{"name":"DEN open","volume":"5 1","pages":""},"PeriodicalIF":1.4000,"publicationDate":"2024-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11208879/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"DEN open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/deo2.396","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
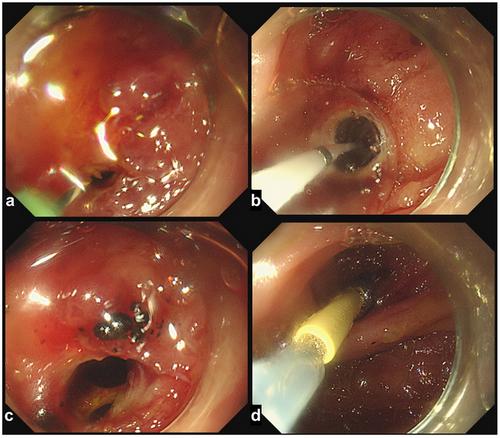
A 79-year-old Japanese woman, who had undergone pancreaticoduodenectomy 6 months prior to presentation owing to pancreatic cancer, complained of jaundice with high fever. Computed tomography revealed proximal bile duct dilatation with complete hepaticojejunostomy anastomotic stricture (HJAS). We performed a single-balloon endoscopy for biliary drainage. The presence of a scar-like feature surrounding the anastomosis was identified as the HJAS. White-light imaging during single-balloon endoscopy revealed that the HJAS contained a milky whitish area (MWA), suggesting that a membranous and fibrosis layer affected continuous inflammation around the center of the anastomosis (within a scar-like feature). Endoscopic dilatation was performed using an endoscopic injection needle, with the MWA used as an indicator. A 23-gauge endoscopic injection needle was used to penetrate the center of the blind lumen within the MWA, and a pinhole was created in the stricture. After confirming the position of the proximal bile duct using a contrast medium with the needle, an endoscopic guidewire with a cannula was inserted into the pinhole. A through-the-scope sequential balloon dilator was used to dilate the stricture, and a plastic stent was inserted into the proximal bile duct. This endoscopic intervention led to positive outcomes. In cases of complete HJAS occlusion, an endoscopic approach to the bile duct is difficult because the anastomotic opening of the HJAS is not visible. Thus, puncturing within the MWA, which can be used as a scar-like landmark within a complete membranous HJAS, is considered a useful endoscopic strategy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


