Innovative solution or cause for concern? The use of continuous glucose monitors in people not living with diabetes: A narrative review
Abstract
Aims
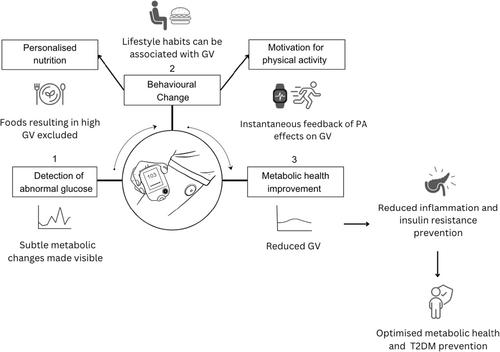
Continuous glucose monitors (CGMs) have expanded their scope beyond indicated uses for diabetes management and are gaining traction among people not living with diabetes (PNLD). CGMs track in time glucose levels and are proposed as tools for the early detection of abnormal glucose and a potential solution for its normalisation through behavioural change, particularly, diet personalisation and motivation of physical activity. This becomes relevance given the growing incidence of metabolic conditions, such as type 2 diabetes mellitus (T2DM). Clinical guidelines, however, do not recommend CGMs in contexts outside type 1 diabetes (T1DM) or insulin-treated T2DM. Therefore, there is a visible disconnect between the indicated and real-world usage of these medical devices. While the commercial market for CGMs in PNLD is expanding rapidly, a comprehensive and evidence-based evaluation of the devices' utility in this population has not been done. Therefore, this review aims to formulate a working model for CGM utility in PNLD as proposed by the ‘health and wellness’ market that advertises and distributes it to these individuals.
Methods
We aim to critically analyse the available research addressing components of the working model, that is (1) detection of abnormal glucose; (2) behavioural change, and (3) metabolic health improvement.
Results
We find a lack of consistent and high-quality evidence to support the utility of CGMs for these purposes. We identify significantly under-reserved areas including clinical benchmarks and scoring procedures for CGM measures, device acceptability, and potential adverse effects of CGMs on eating habits in PNLD. We also raise concerns about the robustness of available CGM research.
Conclusion
In the face of these research gaps, we urge for the commercial claims suggesting the utility of the device in PNLD to be labelled as misleading. We argue that there is a regulatory inadequacy that fuels ‘off-label’ CGM distribution and calls for the strengthening of post-market clinical follow-up oversight for CGMs. We hope this will help to avert the continued misinformation risk to PNLD and ‘off-label’ exacerbation of health disparities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


