Successful Treatment of Steroid-Refractory Immune Thrombocytopenia in a Patient Developing Multiple Myeloma While on Immune Checkpoint Inhibitor Therapy for Lung Cancer: A Case Report.
{"title":"Successful Treatment of Steroid-Refractory Immune Thrombocytopenia in a Patient Developing Multiple Myeloma While on Immune Checkpoint Inhibitor Therapy for Lung Cancer: A Case Report.","authors":"Yudai Hayashi, Masao Tsukada, Daisuke Shinoda, Marina Matsui, Kanichi Iwama, Koichi Kajiwara, Kozai Yasuji","doi":"10.2147/JBM.S468921","DOIUrl":null,"url":null,"abstract":"<p><p>Immune checkpoint inhibitor-related thrombocytopenia (irTCP) is a relatively rare immune-related adverse event (irAE); however, overall survival may worsen when it occurs. Prolonged use of high-dose steroids can diminish the effectiveness of immune checkpoint inhibitor (ICI) therapy on the primary disease because of T lymphocyte suppression, thus early tapering is necessary. We experienced a rare case of a 79-year-old male who concurrently developed irTCP and multiple myeloma (MM) during treatment with ICIs for lung adenocarcinoma. The patient exhibited severe thrombocytopenia and elevated serum IgA levels. Based on various tests, we diagnosed MM and irTCP. Despite administering the standard bortezomib plus dexamethasone (Bd therapy) treatment for MM, there was no response and the irTCP was steroid-resistant. Consequently, we administered a regimen including daratumumab (DPd therapy) for steroid-resistant irTCP and refractory MM, which resulted in a response. As a result, we were able to avoid prolonged use of high-dose steroids and the patient is stable without exacerbation of lung adenocarcinoma for 1 year and 5 months after the onset of MM. To our knowledge, there are no cases of MM developing during ICI treatment and this is the first case report in which daratumumab was effective for the treatment of irTCP.</p>","PeriodicalId":15166,"journal":{"name":"Journal of Blood Medicine","volume":"15 ","pages":"285-290"},"PeriodicalIF":2.7000,"publicationDate":"2024-06-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11198016/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Blood Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/JBM.S468921","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
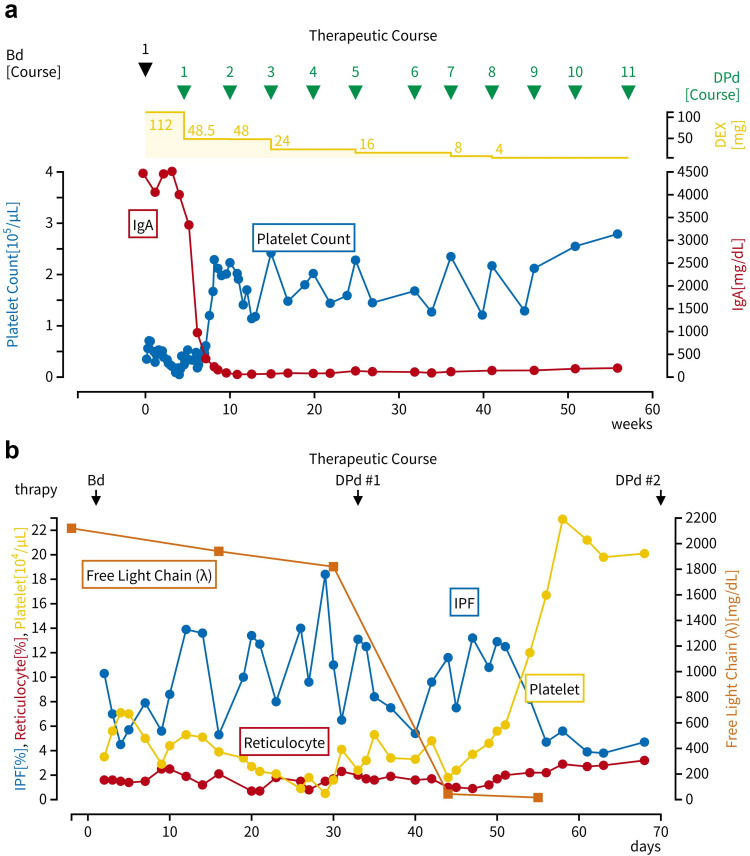
Immune checkpoint inhibitor-related thrombocytopenia (irTCP) is a relatively rare immune-related adverse event (irAE); however, overall survival may worsen when it occurs. Prolonged use of high-dose steroids can diminish the effectiveness of immune checkpoint inhibitor (ICI) therapy on the primary disease because of T lymphocyte suppression, thus early tapering is necessary. We experienced a rare case of a 79-year-old male who concurrently developed irTCP and multiple myeloma (MM) during treatment with ICIs for lung adenocarcinoma. The patient exhibited severe thrombocytopenia and elevated serum IgA levels. Based on various tests, we diagnosed MM and irTCP. Despite administering the standard bortezomib plus dexamethasone (Bd therapy) treatment for MM, there was no response and the irTCP was steroid-resistant. Consequently, we administered a regimen including daratumumab (DPd therapy) for steroid-resistant irTCP and refractory MM, which resulted in a response. As a result, we were able to avoid prolonged use of high-dose steroids and the patient is stable without exacerbation of lung adenocarcinoma for 1 year and 5 months after the onset of MM. To our knowledge, there are no cases of MM developing during ICI treatment and this is the first case report in which daratumumab was effective for the treatment of irTCP.
期刊介绍:
The Journal of Blood Medicine is an international, peer-reviewed, open access, online journal publishing laboratory, experimental and clinical aspects of all topics pertaining to blood based medicine including but not limited to: Transfusion Medicine (blood components, stem cell transplantation, apheresis, gene based therapeutics), Blood collection, Donor issues, Transmittable diseases, and Blood banking logistics, Immunohematology, Artificial and alternative blood based therapeutics, Hematology including disorders/pathology related to leukocytes/immunology, red cells, platelets and hemostasis, Biotechnology/nanotechnology of blood related medicine, Legal aspects of blood medicine, Historical perspectives. Original research, short reports, reviews, case reports and commentaries are invited.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


