Shahab Hajibandeh, Shahin Hajibandeh, Nicholas George Mowbray, Matthew Mortimer, Guy Shingler, Amir Kambal, Bilal Al-Sarireh
{"title":"Minimally invasive versus open central pancreatectomy: A systematic review and meta-analysis.","authors":"Shahab Hajibandeh, Shahin Hajibandeh, Nicholas George Mowbray, Matthew Mortimer, Guy Shingler, Amir Kambal, Bilal Al-Sarireh","doi":"10.14701/ahbps.24-093","DOIUrl":null,"url":null,"abstract":"<p><p>To compare the procedural outcomes of minimally invasive and open central pancreatectomy. A systematic review in compliance with PRISMA statement standards was conducted to identify and analyze studies comparing the procedural outcomes of minimally invasive (laparoscopic or robotic) central pancreatectomy with the open approach. Random effects modeling using intention to treat data, and individual patient as unit of analysis, was used for analyses. Seven comparative studies including 289 patients were included. The two groups were comparable in terms of baseline characteristics. The minimally invasive approach was associated with less intraoperative blood loss (mean difference [MD]: -153.13 mL, <i>p</i> = 0.0004); however, this did not translate into less need for blood transfusion (odds ratio [OR]: 0.30, <i>p</i> = 0.06). The minimally invasive approach resulted in less grade B-C postoperative pancreatic fistula (OR: 0.54, <i>p</i> = 0.03); this did not remain consistent through sensitivity analyses. There was no difference between the two approaches in operative time (MD: 60.17 minutes, <i>p</i> = 0.31), Clavien-Dindo ≥ 3 complications (OR: 1.11, <i>p</i> = 0.78), postoperative mortality (risk difference: -0.00, <i>p</i> = 0.81), and length of stay in hospital (MD: -3.77 days, <i>p</i> = 0.08). Minimally invasive central pancreatectomy may be as safe as the open approach; however, whether it confers advantage over the open approach remains the subject of debate. Type 2 error is a possibility, hence adequately powered studies are required for definite conclusions; future studies may use our data for power analysis.</p>","PeriodicalId":72220,"journal":{"name":"Annals of hepato-biliary-pancreatic surgery","volume":" ","pages":"412-422"},"PeriodicalIF":1.7000,"publicationDate":"2024-11-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11599816/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/ahbps.24-093","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/25 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
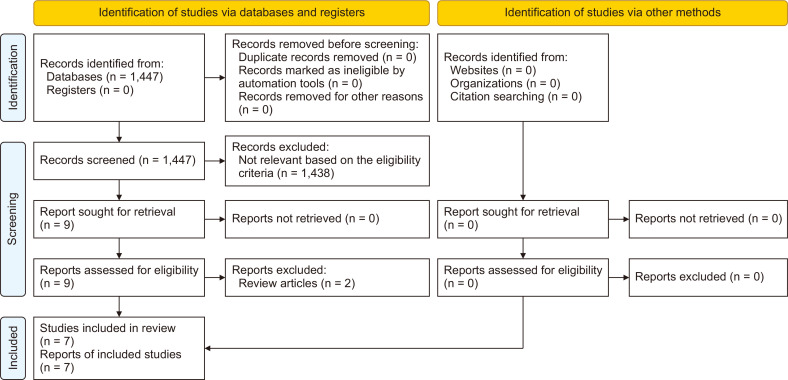
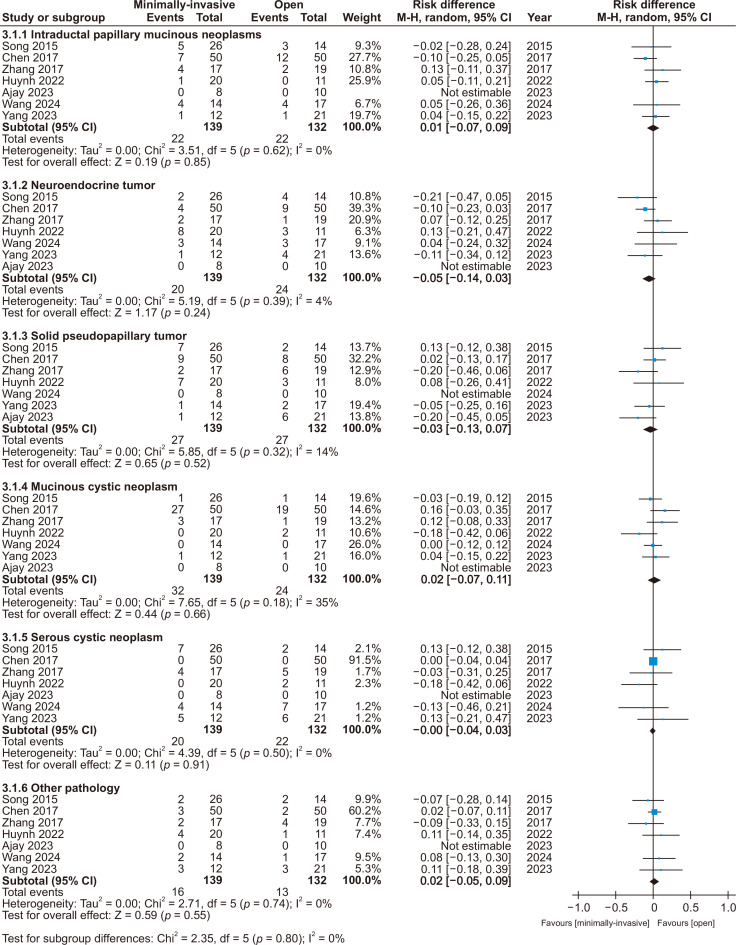
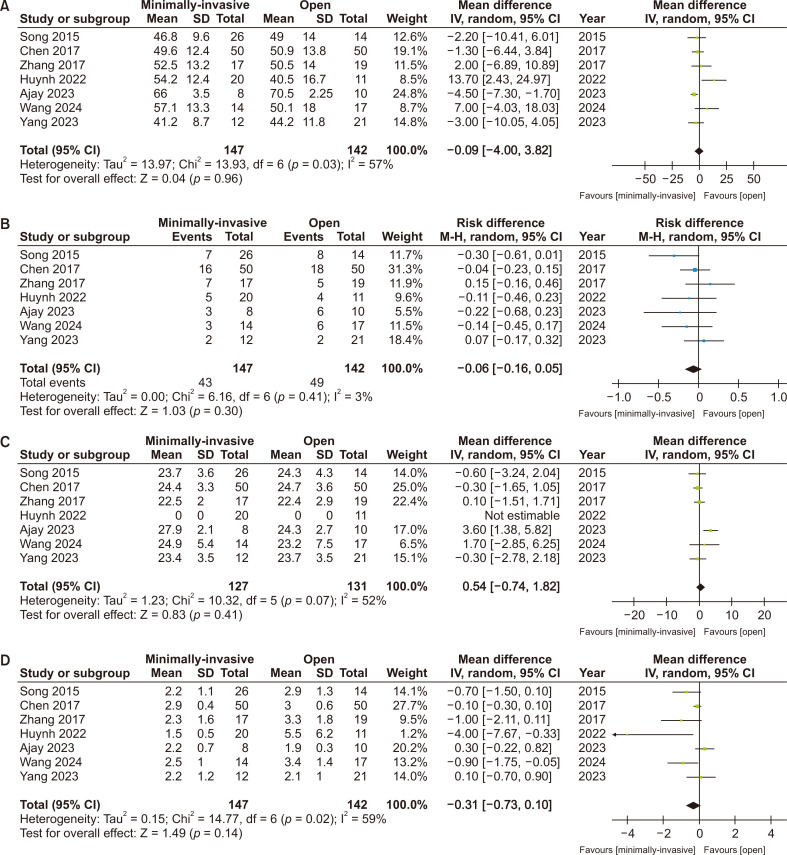
To compare the procedural outcomes of minimally invasive and open central pancreatectomy. A systematic review in compliance with PRISMA statement standards was conducted to identify and analyze studies comparing the procedural outcomes of minimally invasive (laparoscopic or robotic) central pancreatectomy with the open approach. Random effects modeling using intention to treat data, and individual patient as unit of analysis, was used for analyses. Seven comparative studies including 289 patients were included. The two groups were comparable in terms of baseline characteristics. The minimally invasive approach was associated with less intraoperative blood loss (mean difference [MD]: -153.13 mL, p = 0.0004); however, this did not translate into less need for blood transfusion (odds ratio [OR]: 0.30, p = 0.06). The minimally invasive approach resulted in less grade B-C postoperative pancreatic fistula (OR: 0.54, p = 0.03); this did not remain consistent through sensitivity analyses. There was no difference between the two approaches in operative time (MD: 60.17 minutes, p = 0.31), Clavien-Dindo ≥ 3 complications (OR: 1.11, p = 0.78), postoperative mortality (risk difference: -0.00, p = 0.81), and length of stay in hospital (MD: -3.77 days, p = 0.08). Minimally invasive central pancreatectomy may be as safe as the open approach; however, whether it confers advantage over the open approach remains the subject of debate. Type 2 error is a possibility, hence adequately powered studies are required for definite conclusions; future studies may use our data for power analysis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


