Single-center experience of efficacy and safety of atrioventricular node ablation after left bundle branch area pacing for the management of atrial fibrillation.
{"title":"Single-center experience of efficacy and safety of atrioventricular node ablation after left bundle branch area pacing for the management of atrial fibrillation.","authors":"Mathieu Jacobs, Alexandre Bodin, Pascal Spiesser, Dominique Babuty, Nicolas Clementy, Arnaud Bisson","doi":"10.1007/s10840-024-01847-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Atrioventricular node ablation (AVNA) with permanent pacing is an effective treatment of symptomatic atrial fibrillation (AF). Left bundle branch area pacing (LBBAP) prevents cardiac dyssynchrony associated with right ventricular pacing and could prevent worsening of heart failure (HF).</p><p><strong>Methods: </strong>In this retrospective monocentric study, all patients who received AVNA procedure with LBBAP were consecutively included. AVNA procedure data, electrical and echocardiographic parameters at 6 months, and clinical outcomes at 1 year were studied and compared to a matched cohort of patients who received AVNA procedure with conventional pacing between 2010 and 2023.</p><p><strong>Results: </strong>Seventy-five AVNA procedures associated with LBBAP were studied. AVNA in this context was feasible, with a success rate of 98.7% at first ablation, and safe without any complications. There was no threshold rise at follow-up. At 1 year, 6 (8%) patients were hospitalized for HF and 2 (2.7%) were deceased. Patients had a significant improvement in NYHA class and left ventricular ejection fraction (LVEF) (P ≤ 0.0001). When compared to a matched cohort of patients with AVNA and conventional pacing, AVNA data and pacing complications rates were similar. Patients with LBBAP had a better improvement of LVEF (+5.27 ± 9.62% vs. -0.48 ± 14%, P = 0.01), and a lower 1-year rate of composite outcome of hospitalization for HF or death (HR 0.39, 95% CI: 0.16-0.95, P = 0.037), significant on survival analysis (log-rank P-value = 0.03).</p><p><strong>Conclusion: </strong>AVNA with LBBAP in patients with symptomatic AF is feasible, safe, and efficient. Hospitalization for HF or death rate was significantly lower and LVEF improvement was greater.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"1865-1876"},"PeriodicalIF":2.1000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-024-01847-2","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/24 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Atrioventricular node ablation (AVNA) with permanent pacing is an effective treatment of symptomatic atrial fibrillation (AF). Left bundle branch area pacing (LBBAP) prevents cardiac dyssynchrony associated with right ventricular pacing and could prevent worsening of heart failure (HF).
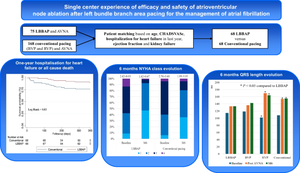
Methods: In this retrospective monocentric study, all patients who received AVNA procedure with LBBAP were consecutively included. AVNA procedure data, electrical and echocardiographic parameters at 6 months, and clinical outcomes at 1 year were studied and compared to a matched cohort of patients who received AVNA procedure with conventional pacing between 2010 and 2023.
Results: Seventy-five AVNA procedures associated with LBBAP were studied. AVNA in this context was feasible, with a success rate of 98.7% at first ablation, and safe without any complications. There was no threshold rise at follow-up. At 1 year, 6 (8%) patients were hospitalized for HF and 2 (2.7%) were deceased. Patients had a significant improvement in NYHA class and left ventricular ejection fraction (LVEF) (P ≤ 0.0001). When compared to a matched cohort of patients with AVNA and conventional pacing, AVNA data and pacing complications rates were similar. Patients with LBBAP had a better improvement of LVEF (+5.27 ± 9.62% vs. -0.48 ± 14%, P = 0.01), and a lower 1-year rate of composite outcome of hospitalization for HF or death (HR 0.39, 95% CI: 0.16-0.95, P = 0.037), significant on survival analysis (log-rank P-value = 0.03).
Conclusion: AVNA with LBBAP in patients with symptomatic AF is feasible, safe, and efficient. Hospitalization for HF or death rate was significantly lower and LVEF improvement was greater.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


