{"title":"D-dimer as a Marker of Severity and Prognosis in Acute Pancreatitis.","authors":"Mario Victor Newton","doi":"10.4103/ijabmr.ijabmr_483_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Acute pancreatitis (AP) scores need a battery of tests that are not helpful at an early stage. Can a single test predict Complicated Acute Pancreatitis (CAP) which includes moderate and severe AP, local complications, and need for intensive care unit (ICU).</p><p><strong>Methodology: </strong>30 patients of AP. D-dimer, C-reactive protein levels done within 3 days of AP onset. APACHE II, Ranson's score, CT severity index were done. Inhospital disease course for development of organ failure and need for ICU care was followed daily.</p><p><strong>Results: </strong>D-dimer in CAP was 2732 ng/L (MAP 567 ng/L), in abnormal computed tomography (CT) was 1916 ng/L (normal CT 363 ng/L), and in organ failure was 4776 ng/L (776.5 ng/L absent organ failure). D-dimer increases as the severity of organ failure increases (<i>P</i> = 0.04). D-dimer in ICU patients was significantly elevated (<i>P</i> = 0.021). D-dimer correlates with APACHE II score well, with an increase in predictive mortality rate (<i>P</i> = 0.01). On receiver operator characteristics, D-dimer >933.5 ng/L predicts CAP, >827.5 ng/L predicts positive CT findings (local complications), and >1060.5 ng/L predicts the development of organ failure.</p><p><strong>Conclusion: </strong>Coagulopathy and microthrombi play a significant role in early pathogenesis. D-dimer test acts at the level of this core pathogenesis, even before the complications set in. D-dimer within 72 h of AP correlates well with the CT findings after 72 h. This is the first study that correlates D-dimer levels with CT scores, ICU requirement. D-dimer can guide primary care physicians in selecting AP patients for referral to a higher center in a resource-limited setting.</p>","PeriodicalId":13727,"journal":{"name":"International Journal of Applied and Basic Medical Research","volume":"14 2","pages":"101-107"},"PeriodicalIF":0.8000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11189266/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Applied and Basic Medical Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ijabmr.ijabmr_483_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/24 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objectives: Acute pancreatitis (AP) scores need a battery of tests that are not helpful at an early stage. Can a single test predict Complicated Acute Pancreatitis (CAP) which includes moderate and severe AP, local complications, and need for intensive care unit (ICU).
Methodology: 30 patients of AP. D-dimer, C-reactive protein levels done within 3 days of AP onset. APACHE II, Ranson's score, CT severity index were done. Inhospital disease course for development of organ failure and need for ICU care was followed daily.
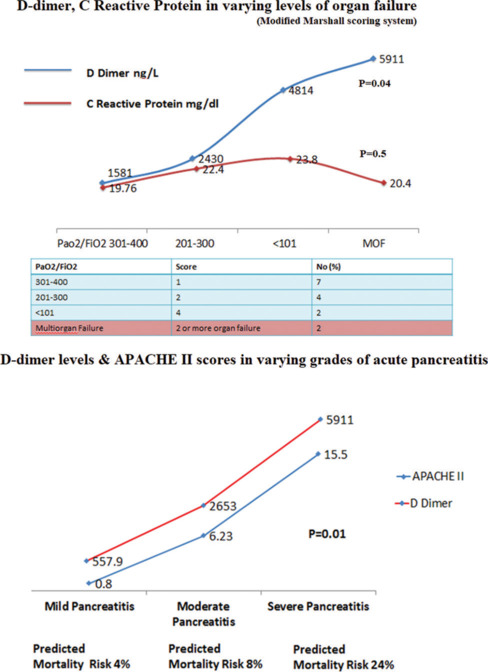
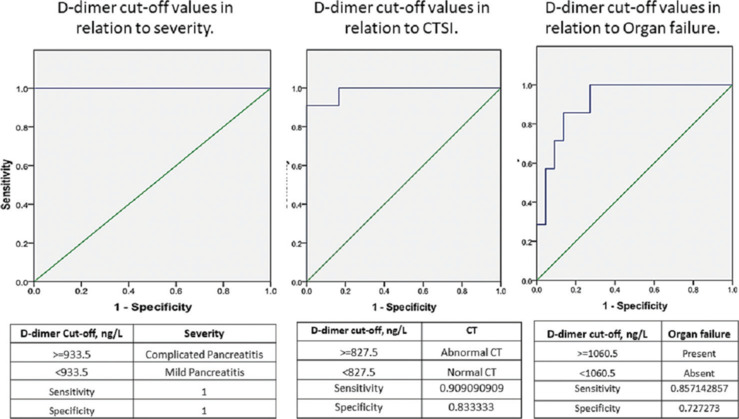
Results: D-dimer in CAP was 2732 ng/L (MAP 567 ng/L), in abnormal computed tomography (CT) was 1916 ng/L (normal CT 363 ng/L), and in organ failure was 4776 ng/L (776.5 ng/L absent organ failure). D-dimer increases as the severity of organ failure increases (P = 0.04). D-dimer in ICU patients was significantly elevated (P = 0.021). D-dimer correlates with APACHE II score well, with an increase in predictive mortality rate (P = 0.01). On receiver operator characteristics, D-dimer >933.5 ng/L predicts CAP, >827.5 ng/L predicts positive CT findings (local complications), and >1060.5 ng/L predicts the development of organ failure.
Conclusion: Coagulopathy and microthrombi play a significant role in early pathogenesis. D-dimer test acts at the level of this core pathogenesis, even before the complications set in. D-dimer within 72 h of AP correlates well with the CT findings after 72 h. This is the first study that correlates D-dimer levels with CT scores, ICU requirement. D-dimer can guide primary care physicians in selecting AP patients for referral to a higher center in a resource-limited setting.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


