A meta-analysis of randomized controlled clinical trials for implications of acute treatment effects on glomerular filtration rate for long-term kidney protection
{"title":"A meta-analysis of randomized controlled clinical trials for implications of acute treatment effects on glomerular filtration rate for long-term kidney protection","authors":"","doi":"10.1016/j.kint.2024.05.024","DOIUrl":null,"url":null,"abstract":"<div><p>Pharmacologic interventions to slow chronic kidney disease progression, such as ACE-inhibitors, angiotensin receptor blockers, or sodium glucose co-transporter 2 inhibitors, often produce acute treatment effects on glomerular filtration rate (GFR) that differ from their long-term chronic treatment effects. Observational studies assessing the implications of acute effects cannot distinguish acute effects from GFR changes unrelated to the treatment. Here, we performed meta-regression analysis of multiple trials to isolate acute effects to determine their long-term implications. In 64 randomized controlled trials (RCTs), enrolling 154,045 participants, we estimated acute effects as the mean between-group difference in GFR slope from baseline to three months, effects on chronic GFR slope (starting at three months after randomization), and effects on three composite kidney endpoints defined by kidney failure (GFR 15 ml/min/1.73m<sup>2</sup> or less, chronic dialysis, or kidney transplantation) or sustained GFR declines of 30%, 40% or 57% decline, respectively. We used Bayesian meta-regression to relate acute effects with treatment effects on chronic slope and the composite kidney endpoints. Overall, acute effects were not associated with treatment effects on chronic slope. Acute effects were associated with the treatment effects on composite kidney outcomes such that larger negative acute effects were associated with lesser beneficial effects on the composite kidney endpoints. Associations were stronger when the kidney composite endpoints were defined by smaller thresholds of GFR decline (30% or 40%). Results were similar in a subgroup of interventions with supposedly hemodynamic effects that acutely reduce GFR. For studies with GFR 60 mL/min/1.73m<sup>2</sup> or under, negative acute effects were associated with larger beneficial effects on chronic GFR slope. Thus, our data from a large and diverse set of RCTs suggests that acute effects of interventions may influence the treatment effect on clinical kidney outcomes.</p></div>","PeriodicalId":17801,"journal":{"name":"Kidney international","volume":null,"pages":null},"PeriodicalIF":14.8000,"publicationDate":"2024-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S0085253824004058/pdfft?md5=30b1beda3a1ec8bafbc3a98e3afaa320&pid=1-s2.0-S0085253824004058-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kidney international","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0085253824004058","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
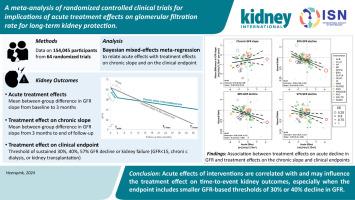
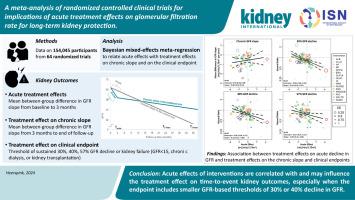
Pharmacologic interventions to slow chronic kidney disease progression, such as ACE-inhibitors, angiotensin receptor blockers, or sodium glucose co-transporter 2 inhibitors, often produce acute treatment effects on glomerular filtration rate (GFR) that differ from their long-term chronic treatment effects. Observational studies assessing the implications of acute effects cannot distinguish acute effects from GFR changes unrelated to the treatment. Here, we performed meta-regression analysis of multiple trials to isolate acute effects to determine their long-term implications. In 64 randomized controlled trials (RCTs), enrolling 154,045 participants, we estimated acute effects as the mean between-group difference in GFR slope from baseline to three months, effects on chronic GFR slope (starting at three months after randomization), and effects on three composite kidney endpoints defined by kidney failure (GFR 15 ml/min/1.73m2 or less, chronic dialysis, or kidney transplantation) or sustained GFR declines of 30%, 40% or 57% decline, respectively. We used Bayesian meta-regression to relate acute effects with treatment effects on chronic slope and the composite kidney endpoints. Overall, acute effects were not associated with treatment effects on chronic slope. Acute effects were associated with the treatment effects on composite kidney outcomes such that larger negative acute effects were associated with lesser beneficial effects on the composite kidney endpoints. Associations were stronger when the kidney composite endpoints were defined by smaller thresholds of GFR decline (30% or 40%). Results were similar in a subgroup of interventions with supposedly hemodynamic effects that acutely reduce GFR. For studies with GFR 60 mL/min/1.73m2 or under, negative acute effects were associated with larger beneficial effects on chronic GFR slope. Thus, our data from a large and diverse set of RCTs suggests that acute effects of interventions may influence the treatment effect on clinical kidney outcomes.
期刊介绍:
Kidney International (KI), the official journal of the International Society of Nephrology, is led by Dr. Pierre Ronco (Paris, France) and stands as one of nephrology's most cited and esteemed publications worldwide.
KI provides exceptional benefits for both readers and authors, featuring highly cited original articles, focused reviews, cutting-edge imaging techniques, and lively discussions on controversial topics.
The journal is dedicated to kidney research, serving researchers, clinical investigators, and practicing nephrologists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


