{"title":"Histopathologic Features of Unmasked Inflammatory Bowel Disease Following Immune Checkpoint Inhibitor Therapy in Colon Biopsies","authors":"","doi":"10.1016/j.gastha.2024.05.011","DOIUrl":null,"url":null,"abstract":"<div><h3>Background and Aims</h3><p>Typical immune checkpoint inhibitor-induced colitis (T-ICI) has significant histomorphologic overlap with inflammatory bowel disease (IBD), a distinction further complicated in ICI-treated patients with pre-existing inflammatory bowel disease (P-IBD) and those with potentially “unmasked” inflammatory bowel disease (U-IBD) after ICI therapy. This study describes histopathologic findings seen in U-IBD colonic biopsies and assesses for distinguishing features from T-ICI and P-IBD biopsies.</p></div><div><h3>Methods</h3><p>Initial colon biopsies after symptom onset from 34 patients on ICI therapy were reviewed, and histopathologic features were tabulated. U-IBD patients were identified clinically based on rapid toxicity development post-ICI treatment with multiple recurrences after immune suppression, frequently with regional colitis (versus pancolitis).</p></div><div><h3>Results</h3><p>The study cohort was classified into T-ICI (n = 20), P-IBD (n = 9), and U-IBD (n = 5) groups. The predominant histological patterns were diffuse active colitis (35%) in the T-ICI, and chronic active colitis in both the P-IBD (67%) and U-IBD (60%) groups (overall <em>P</em> = .003, <em>P</em> > .05 between the two IBD groups). None of the T-ICI biopsies demonstrated chronicity features (ie, architectural distortion score 2, basal lymphoplasmacytosis, or Paneth cell metaplasia). Only U-IBD biopsies demonstrated basal lymphoplasmacytosis (60% vs 0% in T-ICI/P-IBD, <em>P</em> = .002). Among available follow-up biopsies, chronicity features were present in all (4/4) U-IBD patients, including those without chronicity seen in the initial biopsy, but none (0/7) of T-ICI patients.</p></div><div><h3>Conclusion</h3><p>These early results show that no definite features of chronicity were seen in colon biopsies from T-ICI patients, suggesting that the presence of those features may be a clue to U-IBD in patients without a known IBD diagnosis. Frequent basal lymphoplasmacytosis seen in U-IBD may support a recent onset of mucosal injury and early architectural remodeling.</p></div>","PeriodicalId":73130,"journal":{"name":"Gastro hep advances","volume":"3 7","pages":"Pages 986-994"},"PeriodicalIF":0.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2772572324000797/pdfft?md5=ddf2747df63531821784e978adf831b8&pid=1-s2.0-S2772572324000797-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastro hep advances","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2772572324000797","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background and Aims
Typical immune checkpoint inhibitor-induced colitis (T-ICI) has significant histomorphologic overlap with inflammatory bowel disease (IBD), a distinction further complicated in ICI-treated patients with pre-existing inflammatory bowel disease (P-IBD) and those with potentially “unmasked” inflammatory bowel disease (U-IBD) after ICI therapy. This study describes histopathologic findings seen in U-IBD colonic biopsies and assesses for distinguishing features from T-ICI and P-IBD biopsies.
Methods
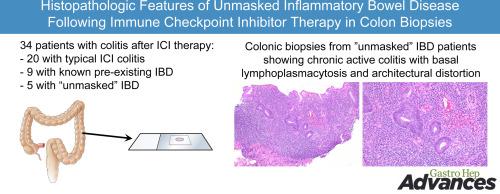
Initial colon biopsies after symptom onset from 34 patients on ICI therapy were reviewed, and histopathologic features were tabulated. U-IBD patients were identified clinically based on rapid toxicity development post-ICI treatment with multiple recurrences after immune suppression, frequently with regional colitis (versus pancolitis).
Results
The study cohort was classified into T-ICI (n = 20), P-IBD (n = 9), and U-IBD (n = 5) groups. The predominant histological patterns were diffuse active colitis (35%) in the T-ICI, and chronic active colitis in both the P-IBD (67%) and U-IBD (60%) groups (overall P = .003, P > .05 between the two IBD groups). None of the T-ICI biopsies demonstrated chronicity features (ie, architectural distortion score 2, basal lymphoplasmacytosis, or Paneth cell metaplasia). Only U-IBD biopsies demonstrated basal lymphoplasmacytosis (60% vs 0% in T-ICI/P-IBD, P = .002). Among available follow-up biopsies, chronicity features were present in all (4/4) U-IBD patients, including those without chronicity seen in the initial biopsy, but none (0/7) of T-ICI patients.
Conclusion
These early results show that no definite features of chronicity were seen in colon biopsies from T-ICI patients, suggesting that the presence of those features may be a clue to U-IBD in patients without a known IBD diagnosis. Frequent basal lymphoplasmacytosis seen in U-IBD may support a recent onset of mucosal injury and early architectural remodeling.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


