Immunosuppression with cyclosporine versus tacrolimus shows distinctive nephrotoxicity profiles within renal compartments
Abstract
Aim
Calcineurin inhibitors (CNIs) are the backbone for immunosuppression after solid organ transplantation. Although successful in preventing kidney transplant rejection, their nephrotoxic side effects contribute to allograft injury. Renal parenchymal lesions occur for cyclosporine A (CsA) as well as for the currently favored tacrolimus (Tac). We aimed to study whether chronic CsA and Tac exposures, before reaching irreversible nephrotoxic damage, affect renal compartments differentially and whether related pathogenic mechanisms can be identified.
Methods
CsA and Tac were administered chronically in wild type Wistar rats using osmotic minipumps over 4 weeks. Functional parameters were controlled. Electron microscopy, confocal, and 3D-structured illumination microscopy were used for histopathology. Clinical translatability was tested in human renal biopsies. Standard biochemical, RNA-seq, and proteomic technologies were applied to identify implicated molecular pathways.
Results
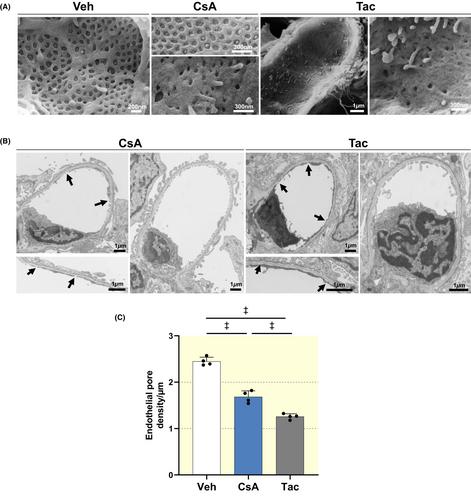
Both drugs caused significant albeit differential damage in vasculature and nephron. The glomerular filtration barrier was more affected by Tac than by CsA, showing prominent deteriorations in endothelium and podocytes along with impaired VEGF/VEGFR2 signaling and podocyte-specific gene expression. By contrast, proximal tubule epithelia were more severely affected by CsA than by Tac, revealing lysosomal dysfunction, enhanced apoptosis, impaired proteostasis and oxidative stress. Lesion characteristics were confirmed in human renal biopsies.
Conclusion
We conclude that pathogenetic alterations in the renal compartments are specific for either treatment. Considering translation to the clinical setting, CNI choice should reflect individual risk factors for renal vasculature and tubular epithelia. As a step in this direction, we share protein signatures identified from multiomics with potential pathognomonic relevance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


