Guillaume Pouessel, Timothy E. Dribin, Charles Tacquard, Luciana Kase Tanno, Victoria Cardona, Margitta Worm, Antoine Deschildre, Antonella Muraro, Lene H. Garvey, Paul J. Turner
{"title":"Management of Refractory Anaphylaxis: An Overview of Current Guidelines","authors":"Guillaume Pouessel, Timothy E. Dribin, Charles Tacquard, Luciana Kase Tanno, Victoria Cardona, Margitta Worm, Antoine Deschildre, Antonella Muraro, Lene H. Garvey, Paul J. Turner","doi":"10.1111/cea.14514","DOIUrl":null,"url":null,"abstract":"<p>In this review, we compare different refractory anaphylaxis (RA) management guidelines focusing on cardiovascular involvement and best practice recommendations, discuss postulated pathogenic mechanisms underlining RA and highlight knowledge gaps and research priorities. There is a paucity of data supporting existing management guidelines. Therapeutic recommendations include the need for the timely administration of appropriate doses of aggressive fluid resuscitation and intravenous (IV) adrenaline in RA. The preferred second-line vasopressor (noradrenaline, vasopressin, metaraminol and dopamine) is unknown. Most guidelines recommend IV glucagon for patients on beta-blockers, despite a lack of evidence. The use of methylene blue or extracorporeal life support (ECLS) is also suggested as rescue therapy. Despite recent advances in understanding the pathogenesis of anaphylaxis, the factors that lead to a lack of response to the initial adrenaline and thus RA are unclear. Genetic factors, such as deficiency in platelet activating factor-acetyl hydrolase or hereditary alpha-tryptasaemia, mastocytosis may modulate reaction severity or response to treatment. Further research into the underlying pathophysiology of RA may help define potential new therapeutic approaches and reduce the morbidity and mortality of anaphylaxis.</p>","PeriodicalId":10207,"journal":{"name":"Clinical and Experimental Allergy","volume":"54 7","pages":"470-488"},"PeriodicalIF":6.3000,"publicationDate":"2024-06-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cea.14514","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cea.14514","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
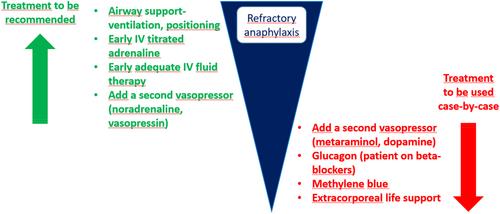
In this review, we compare different refractory anaphylaxis (RA) management guidelines focusing on cardiovascular involvement and best practice recommendations, discuss postulated pathogenic mechanisms underlining RA and highlight knowledge gaps and research priorities. There is a paucity of data supporting existing management guidelines. Therapeutic recommendations include the need for the timely administration of appropriate doses of aggressive fluid resuscitation and intravenous (IV) adrenaline in RA. The preferred second-line vasopressor (noradrenaline, vasopressin, metaraminol and dopamine) is unknown. Most guidelines recommend IV glucagon for patients on beta-blockers, despite a lack of evidence. The use of methylene blue or extracorporeal life support (ECLS) is also suggested as rescue therapy. Despite recent advances in understanding the pathogenesis of anaphylaxis, the factors that lead to a lack of response to the initial adrenaline and thus RA are unclear. Genetic factors, such as deficiency in platelet activating factor-acetyl hydrolase or hereditary alpha-tryptasaemia, mastocytosis may modulate reaction severity or response to treatment. Further research into the underlying pathophysiology of RA may help define potential new therapeutic approaches and reduce the morbidity and mortality of anaphylaxis.
在这篇综述中,我们比较了不同的难治性过敏性休克(RA)管理指南,重点关注心血管参与和最佳实践建议,讨论了RA的假设致病机制,并强调了知识差距和研究重点。支持现有管理指南的数据很少。治疗建议包括:RA 患者需要及时给予适当剂量的积极液体复苏和静脉注射肾上腺素。首选的二线血管加压药(去甲肾上腺素、血管加压素、美他明醇和多巴胺)尚不明确。尽管缺乏证据,但大多数指南都建议使用β受体阻滞剂的患者静脉注射胰高血糖素。此外,还建议使用亚甲蓝或体外生命支持(ECLS)作为抢救疗法。尽管最近在了解过敏性休克的发病机制方面取得了进展,但导致对初始肾上腺素缺乏反应并进而导致 RA 的因素仍不清楚。遗传因素,如血小板活化因子乙酰水解酶缺乏或遗传性α-色氨酸血症、肥大细胞增多症可能会影响反应的严重程度或对治疗的反应。对 RA 潜在病理生理学的进一步研究可能有助于确定潜在的新治疗方法,降低过敏性休克的发病率和死亡率。
期刊介绍:
Clinical & Experimental Allergy strikes an excellent balance between clinical and scientific articles and carries regular reviews and editorials written by leading authorities in their field.
In response to the increasing number of quality submissions, since 1996 the journals size has increased by over 30%. Clinical & Experimental Allergy is essential reading for allergy practitioners and research scientists with an interest in allergic diseases and mechanisms. Truly international in appeal, Clinical & Experimental Allergy publishes clinical and experimental observations in disease in all fields of medicine in which allergic hypersensitivity plays a part.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


