Yang Chen, Ying Gue, Maciej Banach, Dimitri Mikhailidis, Peter P. Toth, Marek Gierlotka, Tadeusz Osadnik, Marcin Golawski, Tomasz Tomasik, Adam Windak, Jacek Jozwiak, Gregory Y. H. Lip, the LIPIDOGRAM Investigators
{"title":"Phenotypes of Polish primary care patients using hierarchical clustering: Exploring the risk of mortality in the LIPIDOGEN2015 study cohort","authors":"Yang Chen, Ying Gue, Maciej Banach, Dimitri Mikhailidis, Peter P. Toth, Marek Gierlotka, Tadeusz Osadnik, Marcin Golawski, Tomasz Tomasik, Adam Windak, Jacek Jozwiak, Gregory Y. H. Lip, the LIPIDOGRAM Investigators","doi":"10.1111/eci.14261","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Comorbidities in primary care do not occur in isolation but tend to cluster together causing various clinically complex phenotypes. This study aimed to distinguish phenotype clusters and identify the risks of all-cause mortality in primary care.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>The baseline cohort of the LIPIDOGEN2015 sub-study involved 1779 patients recruited by 438 primary care physicians. To identify different phenotype clusters, we used hierarchical clustering and investigated differences between clinical characteristics and mortality between clusters. We then performed causal analyses using causal mediation analysis to explore potential mediators between different clusters and all-cause mortality.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 1756 patients were included (mean age 51.2, SD 13.0; 60.3% female), with a median follow-up of 5.7 years. Three clusters were identified: Cluster 1 (<i>n</i> = 543) was characterised by overweight/obesity (body mass index ≥ 25 kg/m<sup>2</sup>), older (age ≥ 65 years), more comorbidities; Cluster 2 (<i>n</i> = 459) was characterised by non-overweight/obesity, younger, fewer comorbidities; Cluster 3 (<i>n</i> = 754) was characterised by overweight/obesity, younger, fewer comorbidities. Adjusted Cox regression showed that compared with Cluster 2, Cluster 1 had a significantly higher risk of all-cause mortality (HR 3.87, 95% CI: 1.24–15.91), whereas this was insignificantly different for Cluster 3. Causal mediation analyses showed that decreased protein thiol groups mediated the hazard effect of all-cause mortality in Cluster 1 compared with Cluster 2, but not between Clusters 1 and 3.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Overweight/obesity older patients with more comorbidities had the highest risk of long-term all-cause mortality, and in the young group population overweight/obesity insignificantly increased the risk in the long-term follow-up, providing a basis for stratified phenotypic risk management.</p>\n </section>\n </div>","PeriodicalId":12013,"journal":{"name":"European Journal of Clinical Investigation","volume":"54 10","pages":""},"PeriodicalIF":4.4000,"publicationDate":"2024-06-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/eci.14261","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Clinical Investigation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/eci.14261","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Comorbidities in primary care do not occur in isolation but tend to cluster together causing various clinically complex phenotypes. This study aimed to distinguish phenotype clusters and identify the risks of all-cause mortality in primary care.
Methods
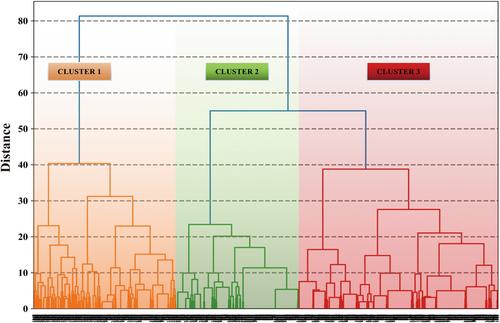
The baseline cohort of the LIPIDOGEN2015 sub-study involved 1779 patients recruited by 438 primary care physicians. To identify different phenotype clusters, we used hierarchical clustering and investigated differences between clinical characteristics and mortality between clusters. We then performed causal analyses using causal mediation analysis to explore potential mediators between different clusters and all-cause mortality.
Results
A total of 1756 patients were included (mean age 51.2, SD 13.0; 60.3% female), with a median follow-up of 5.7 years. Three clusters were identified: Cluster 1 (n = 543) was characterised by overweight/obesity (body mass index ≥ 25 kg/m2), older (age ≥ 65 years), more comorbidities; Cluster 2 (n = 459) was characterised by non-overweight/obesity, younger, fewer comorbidities; Cluster 3 (n = 754) was characterised by overweight/obesity, younger, fewer comorbidities. Adjusted Cox regression showed that compared with Cluster 2, Cluster 1 had a significantly higher risk of all-cause mortality (HR 3.87, 95% CI: 1.24–15.91), whereas this was insignificantly different for Cluster 3. Causal mediation analyses showed that decreased protein thiol groups mediated the hazard effect of all-cause mortality in Cluster 1 compared with Cluster 2, but not between Clusters 1 and 3.
Conclusion
Overweight/obesity older patients with more comorbidities had the highest risk of long-term all-cause mortality, and in the young group population overweight/obesity insignificantly increased the risk in the long-term follow-up, providing a basis for stratified phenotypic risk management.
期刊介绍:
EJCI considers any original contribution from the most sophisticated basic molecular sciences to applied clinical and translational research and evidence-based medicine across a broad range of subspecialties. The EJCI publishes reports of high-quality research that pertain to the genetic, molecular, cellular, or physiological basis of human biology and disease, as well as research that addresses prevalence, diagnosis, course, treatment, and prevention of disease. We are primarily interested in studies directly pertinent to humans, but submission of robust in vitro and animal work is also encouraged. Interdisciplinary work and research using innovative methods and combinations of laboratory, clinical, and epidemiological methodologies and techniques is of great interest to the journal. Several categories of manuscripts (for detailed description see below) are considered: editorials, original articles (also including randomized clinical trials, systematic reviews and meta-analyses), reviews (narrative reviews), opinion articles (including debates, perspectives and commentaries); and letters to the Editor.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


