[Effectiveness of the CNIC polypill in secondary cardiovascular prevention in the subgroup of patients of the NEPTUNO study using atorvastatin doses of 20 mg].
José R González-Juanatey, Alberto Cordero, Luis Masana, Regina Dalmau
{"title":"[Effectiveness of the CNIC polypill in secondary cardiovascular prevention in the subgroup of patients of the NEPTUNO study using atorvastatin doses of 20 mg].","authors":"José R González-Juanatey, Alberto Cordero, Luis Masana, Regina Dalmau","doi":"10.24875/ACM.23000230","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To analyse the incidence and risk of recurrent major adverse cardiovascular events (MACE), level of risk factor control, treatment persistence and cost of the CNIC polypill version containing acetylsalicylic acid (ASA) 100 mg, atorvastatin 20 mg (A20), and ramipril 2.5, 5.0 or 10 mg in secondary cardiovascular prevention patients.</p><p><strong>Method: </strong>Subanalysis of the observational, retrospective, multicentre, NEPTUNO study in patients treated for two years with the CNIC polypill A20, the same monocomponents as single drugs, equipotent drugs, and other therapies.</p><p><strong>Results: </strong>922 patients were included in each group. The risk of recurrent MACE was lower among CNIC A20 polypill users than all others (21%, 23% and 26% increased risk among the monocomponents, equipotent or other therapy cohorts, respectively; p < 0.05). The magnitude of the mean change in low-density lipoprotein cholesterol and blood pressure, as well as the increase in the proportion of patients achieving target goals, was also greater among patients treated with the CNIC A20 polypill than in any of the other cohorts (all p < 0.001). Treatment persistence was significantly higher in patients treated with the CNIC A20 polypill (p < 0.001) and was a less costly strategy than any other therapeutic option.</p><p><strong>Conclusions: </strong>In patients in secondary cardiovascular prevention, the CNIC A20 polypill (ASA 100 mg, atorvastatin 20 mg, and ramipril 2.5, 5.0 or 10 mg) constitutes a valid therapeutic option with similar benefits and outcomes to the version of the polypill with atorvastatin 40 mg.</p>","PeriodicalId":93885,"journal":{"name":"Archivos de cardiologia de Mexico","volume":" ","pages":"429-443"},"PeriodicalIF":0.0000,"publicationDate":"2024-06-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12148536/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archivos de cardiologia de Mexico","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.24875/ACM.23000230","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To analyse the incidence and risk of recurrent major adverse cardiovascular events (MACE), level of risk factor control, treatment persistence and cost of the CNIC polypill version containing acetylsalicylic acid (ASA) 100 mg, atorvastatin 20 mg (A20), and ramipril 2.5, 5.0 or 10 mg in secondary cardiovascular prevention patients.
Method: Subanalysis of the observational, retrospective, multicentre, NEPTUNO study in patients treated for two years with the CNIC polypill A20, the same monocomponents as single drugs, equipotent drugs, and other therapies.
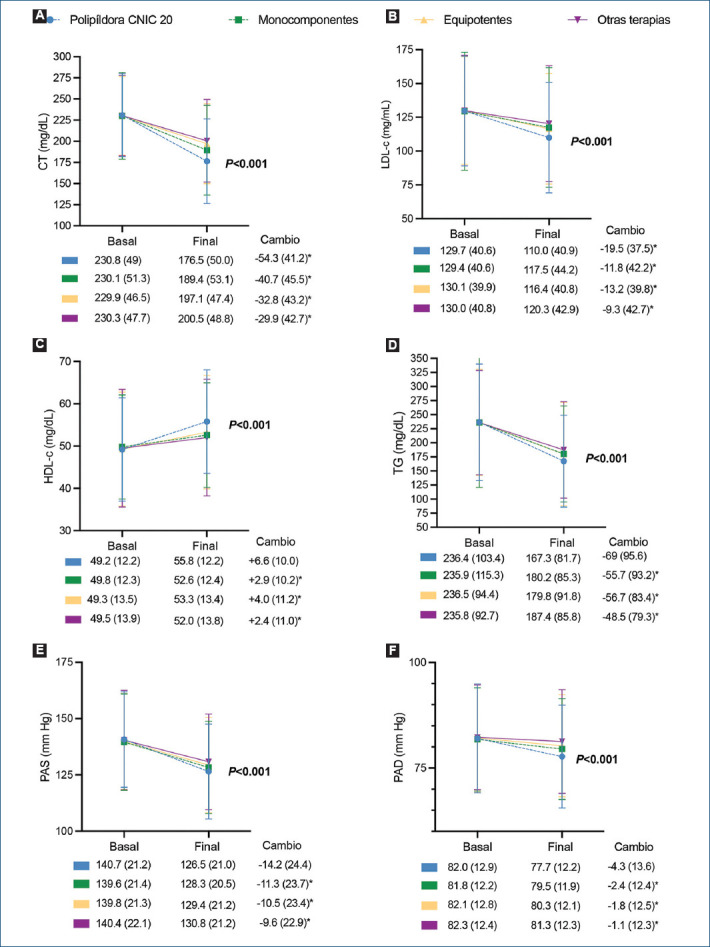
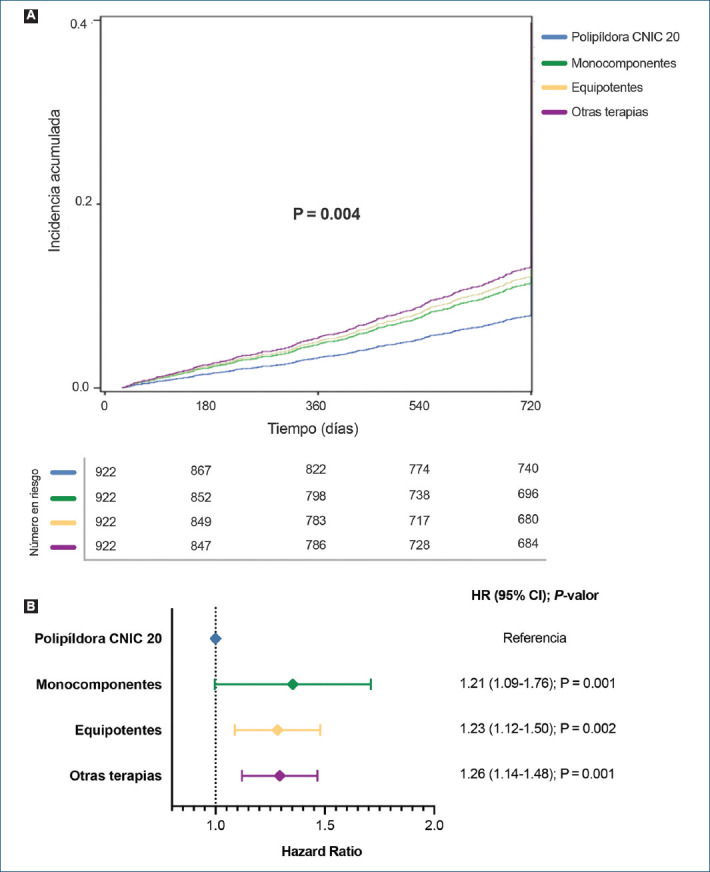
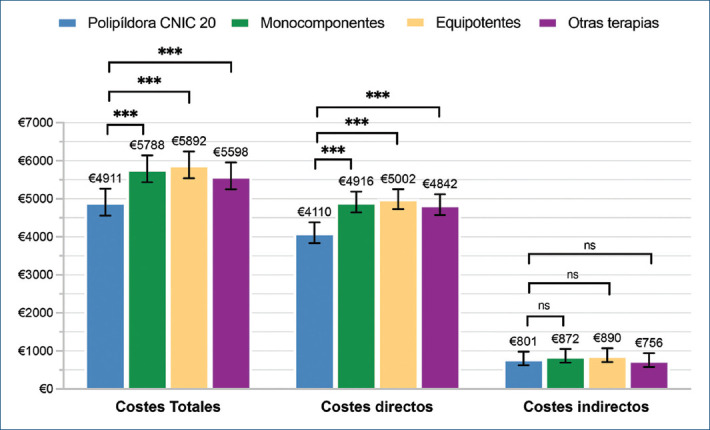
Results: 922 patients were included in each group. The risk of recurrent MACE was lower among CNIC A20 polypill users than all others (21%, 23% and 26% increased risk among the monocomponents, equipotent or other therapy cohorts, respectively; p < 0.05). The magnitude of the mean change in low-density lipoprotein cholesterol and blood pressure, as well as the increase in the proportion of patients achieving target goals, was also greater among patients treated with the CNIC A20 polypill than in any of the other cohorts (all p < 0.001). Treatment persistence was significantly higher in patients treated with the CNIC A20 polypill (p < 0.001) and was a less costly strategy than any other therapeutic option.
Conclusions: In patients in secondary cardiovascular prevention, the CNIC A20 polypill (ASA 100 mg, atorvastatin 20 mg, and ramipril 2.5, 5.0 or 10 mg) constitutes a valid therapeutic option with similar benefits and outcomes to the version of the polypill with atorvastatin 40 mg.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


