Alice Khalil RN, Marisa Bruno RN, Alessandro Spano MSN, Fabrizio Petrone MSN, Edoardo Ghiani RN, Giuseppe Cosma RN, Giuseppe Chiacchio MD, Rocco Simone Flammia MD
{"title":"The pivotal role of the robotic nurse in the management of the robotic urologic surgical environment","authors":"Alice Khalil RN, Marisa Bruno RN, Alessandro Spano MSN, Fabrizio Petrone MSN, Edoardo Ghiani RN, Giuseppe Cosma RN, Giuseppe Chiacchio MD, Rocco Simone Flammia MD","doi":"10.1111/ijun.12400","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction and Objectives</h3>\n \n <p>Robotic surgery has revolutionized urology. However, upfront costs, time investments and knowledge required to proficiently operate and maintain robotic equipment and supplies often make it advantageous to implement the role of dedicated robotic nurse (DN) teams. Herein, we aimed to investigate the impact of DN on operative times during robotic urological procedures.</p>\n </section>\n \n <section>\n \n <h3> Materials and Methods</h3>\n \n <p>We retrospectively identified consecutive robotic uro-oncological procedures performed at our institution from Jan to Oct 2023. The cohort was stratified based on the presence or absence of a DN team (DN vs no-DN). The DN team was defined as having independently managed ≥100 robotic urological procedures. Endpoints were preoperative nursing time (pre-NT), postoperative nursing time (post-NT), surgeon operative time (surg-OT), and total operative time (t-OT). Continuous variables were compared using Student's <i>t</i>-test. Subgroup analyses were conducted for specific procedures: robot-assisted radical cystectomy (RARC), radical prostatectomy (RARP), partial nephrectomy (RAPN), and radical nephrectomy (RARN).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Overall, 421 procedures were included. The DN group exhibited shorter pre-NT (13.5 vs 23.7, <i>p</i> < 0.001), post-NT (12.2 vs. 15, <i>p</i> < 0.001), surg-OT (117 vs. 136, <i>p</i> < 0.001), and t-OT (143.2 vs. 174.9, <i>p</i> < 0.001) compared to the no-DN group. Subgroup analysis revealed shorter pre-NT in the DN group for all procedures: RARP (13.2 vs. 23.5, <i>p</i> < 0.001), RARC (16.4 vs. 29.2, <i>p</i> < 0.001), RARN (12.6 vs. 18.9, <i>p</i> < 0.001) and RAPN (12.7 vs. 20.8, <i>p</i> < 0.001). Conversely, DN group exhibited shorter post-NT in RARP (12 vs. 15.8, <i>p</i> < 0.001) and RARN (12.4 vs. 15.3, <i>p</i>: 0.01), but not in RARC (13 vs. 15, <i>p</i>: 0.06) and RAPN (12.2 vs. 12.7, <i>p</i>: 0.4) subgroup. Similarly, DN group demonstrated shorter t-OT in RARP (162.7 vs. 185.4, <i>p</i> < 0.001), but not in RARC (232.8 vs. 245, <i>p</i>: 0.44), RAPN (91.2 vs. 107.4, <i>p</i>: 0.35) and RARN (118.5 vs. 127.2, <i>p</i>: 0.4) subgroups. Finally, no differences in surg-OT were recorded between the DN and non-DN groups for any of the individual procedures (Table 1; Figure 1).</p>\n \n <div>\n \n \n \n \n <header><span>TABLE 1.\n </span>Comparison of time per procedures between dedicated and non-dedicated teams.</header>\n \n \n \n <div>\n <table>\n \n \n \n \n \n \n \n \n \n \n \n \n \n <thead>\n \n <tr>\n \n <th>Variables mean (SD)</th>\n \n <th>RAPN group</th>\n \n <th>Variables mean (SD)</th>\n \n <th>RARP group</th>\n \n <th>Variables mean (SD)</th>\n \n <th>Overall procedures</th>\n </tr>\n \n <tr>\n \n <th>Dedicated nurse team (86)</th>\n \n <th>No dedicated nurse team (35)</th>\n \n <th><i>p</i>-value</th>\n \n <th>Dedicated nurse team (86)</th>\n \n <th>No dedicated nurse team (35)</th>\n \n <th><i>p</i>-value</th>\n \n <th>Dedicated nurse team (86)</th>\n \n <th>No dedicated nurse team (35)</th>\n \n <th><i>p</i>-value</th>\n </tr>\n </thead>\n \n <tbody>\n \n <tr>\n \n <td>Preoperative nursing time</td>\n \n <td>12.7 (±2.7)</td>\n \n <td>20.8 (±5.9)</td>\n \n <td><b><0</b>.<b>001</b></td>\n \n <td>Preoperative nursing time</td>\n \n <td>13.2 (±3.3)</td>\n \n <td>23.5 (±9.8)</td>\n \n <td><b><0</b>.<b>001</b></td>\n \n <td>Preoperative nursing time</td>\n \n <td>13.5 (±3.6)</td>\n \n <td>23.7 (±9.7)</td>\n \n <td><b><0</b>.<b>001</b></td>\n </tr>\n \n <tr>\n \n <td>Postoperative nursing time</td>\n \n <td>12.2 (±3.7)</td>\n \n <td>12.7 (±3.4)</td>\n \n <td>0.4</td>\n \n <td>Postoperative nursing time</td>\n \n <td>12 (±4.1)</td>\n \n <td>15.8 (±6.3)</td>\n \n <td><0.001</td>\n \n <td>Postoperative nursing time</td>\n \n <td>12.2 (±3.9)</td>\n \n <td>15 (±5.6)</td>\n \n <td><0.001</td>\n </tr>\n \n <tr>\n \n <td>Operative time</td>\n \n <td>66.2 (±29.1)</td>\n \n <td>73.8 (±44.4)</td>\n \n <td>0.3</td>\n \n <td>Operative time</td>\n \n <td>137.5 (±37.2)</td>\n \n <td>146.1 (±41.1)</td>\n \n <td>0.18</td>\n \n <td>Operative time</td>\n \n <td>117 (±68)</td>\n \n <td>136 (±68.8)</td>\n \n <td><b><0</b>.<b>001</b></td>\n </tr>\n \n <tr>\n \n <td>Total operation time</td>\n \n <td>91.2 (±30.2)</td>\n \n <td>107.4 (±46.1)</td>\n \n <td>0.35</td>\n \n <td>Total operation time</td>\n \n <td>162.7 (±37.8)</td>\n \n <td>185.4 (±39.6)</td>\n \n <td><b><0</b>.<b>001</b></td>\n \n <td>Total operation time</td>\n \n <td>143.2 (±69)</td>\n \n <td>174.9 (±72,1)</td>\n \n <td><b><0</b>.<b>001</b></td>\n </tr>\n </tbody>\n </table>\n </div>\n \n <div>\n <table>\n \n \n \n \n \n \n \n \n \n <thead>\n \n <tr>\n \n <th>Variables mean (SD)</th>\n \n <th>RARC group</th>\n \n <th>Variables mean (SD)</th>\n \n <th>RARN group</th>\n </tr>\n \n <tr>\n \n <th>Dedicated nurse team (86)</th>\n \n <th>No dedicated nurse team (35)</th>\n \n <th><i>p</i>-value</th>\n \n <th>Dedicated nurse team (86)</th>\n \n <th>No dedicated nurse team (35)</th>\n \n <th><i>p</i>-value</th>\n </tr>\n </thead>\n \n <tbody>\n \n <tr>\n \n <td>Preoperative nursing time</td>\n \n <td>16.4 (±4.8)</td>\n \n <td>29.2 (±8.9)</td>\n \n <td><b><0</b>.<b>001</b></td>\n \n <td>Preoperative nursing time</td>\n \n <td>12.6 (±2.8)</td>\n \n <td>18.9 (±4.7)</td>\n \n <td><b><0</b>.<b>001</b></td>\n </tr>\n \n <tr>\n \n <td>Postoperative nursing time</td>\n \n <td>13 (±3.5)</td>\n \n <td>15 (±4.5)</td>\n \n <td>0.06</td>\n \n <td>Postoperative nursing time</td>\n \n <td>12.4 (±3.9)</td>\n \n <td>15.3 (±5.7)</td>\n \n <td><b>0.01</b></td>\n </tr>\n \n <tr>\n \n <td>Operative time</td>\n \n <td>203.4 (±68.5)</td>\n \n <td>200.8 (±69.7)</td>\n \n <td>0.86</td>\n \n <td>Operative time</td>\n \n <td>93.5 (±38.7)</td>\n \n <td>93 (±42.2)</td>\n \n <td>0.9</td>\n </tr>\n \n <tr>\n \n <td>Total operation time</td>\n \n <td>232.8 (±66.4)</td>\n \n <td>245 (±72.6)</td>\n \n <td>0.44</td>\n \n <td>Total operation time</td>\n \n <td>118.5 (±38.9)</td>\n \n <td>127.2 (±43.1)</td>\n \n <td>0.4</td>\n </tr>\n </tbody>\n </table>\n </div>\n \n \n \n <div>\n <ul>\n <li>\n <i>Note:</i> Bold indicates significant value.\n </li>\n </ul>\n </div>\n <div></div>\n </div>\n \n <section>\n <figure><picture>\n <source></source></picture><figcaption>\n <div><strong>FIGURE 1<span></span></strong><div>Open in figure viewer<i></i><span>PowerPoint</span></div>\n </div>\n <div>Comparison of preoperative nursing time DN Team versus NoDN Team.</div>\n </figcaption>\n </figure>\n </section>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Our study suggests that the implementation of a dedicated robotic nursing team can lead to substantial reductions in overall operative time. This benefit is primarily attributed to shorter preoperative nursing times, highlighting the crucial role of the robotic nurse in optimizing the robotic surgical environment.</p>\n </section>\n </div>","PeriodicalId":50281,"journal":{"name":"International Journal of Urological Nursing","volume":"18 2","pages":""},"PeriodicalIF":0.5000,"publicationDate":"2024-06-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Urological Nursing","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ijun.12400","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"NURSING","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction and Objectives
Robotic surgery has revolutionized urology. However, upfront costs, time investments and knowledge required to proficiently operate and maintain robotic equipment and supplies often make it advantageous to implement the role of dedicated robotic nurse (DN) teams. Herein, we aimed to investigate the impact of DN on operative times during robotic urological procedures.
Materials and Methods
We retrospectively identified consecutive robotic uro-oncological procedures performed at our institution from Jan to Oct 2023. The cohort was stratified based on the presence or absence of a DN team (DN vs no-DN). The DN team was defined as having independently managed ≥100 robotic urological procedures. Endpoints were preoperative nursing time (pre-NT), postoperative nursing time (post-NT), surgeon operative time (surg-OT), and total operative time (t-OT). Continuous variables were compared using Student's t-test. Subgroup analyses were conducted for specific procedures: robot-assisted radical cystectomy (RARC), radical prostatectomy (RARP), partial nephrectomy (RAPN), and radical nephrectomy (RARN).
Results
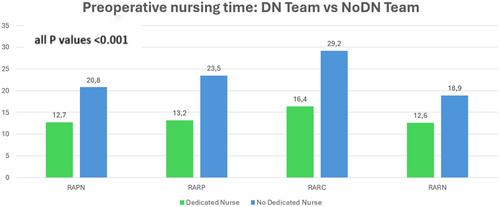
Overall, 421 procedures were included. The DN group exhibited shorter pre-NT (13.5 vs 23.7, p < 0.001), post-NT (12.2 vs. 15, p < 0.001), surg-OT (117 vs. 136, p < 0.001), and t-OT (143.2 vs. 174.9, p < 0.001) compared to the no-DN group. Subgroup analysis revealed shorter pre-NT in the DN group for all procedures: RARP (13.2 vs. 23.5, p < 0.001), RARC (16.4 vs. 29.2, p < 0.001), RARN (12.6 vs. 18.9, p < 0.001) and RAPN (12.7 vs. 20.8, p < 0.001). Conversely, DN group exhibited shorter post-NT in RARP (12 vs. 15.8, p < 0.001) and RARN (12.4 vs. 15.3, p: 0.01), but not in RARC (13 vs. 15, p: 0.06) and RAPN (12.2 vs. 12.7, p: 0.4) subgroup. Similarly, DN group demonstrated shorter t-OT in RARP (162.7 vs. 185.4, p < 0.001), but not in RARC (232.8 vs. 245, p: 0.44), RAPN (91.2 vs. 107.4, p: 0.35) and RARN (118.5 vs. 127.2, p: 0.4) subgroups. Finally, no differences in surg-OT were recorded between the DN and non-DN groups for any of the individual procedures (Table 1; Figure 1).
TABLE 1.
Comparison of time per procedures between dedicated and non-dedicated teams.
Variables mean (SD)
RAPN group
Variables mean (SD)
RARP group
Variables mean (SD)
Overall procedures
Dedicated nurse team (86)
No dedicated nurse team (35)
p-value
Dedicated nurse team (86)
No dedicated nurse team (35)
p-value
Dedicated nurse team (86)
No dedicated nurse team (35)
p-value
Preoperative nursing time
12.7 (±2.7)
20.8 (±5.9)
<0.001
Preoperative nursing time
13.2 (±3.3)
23.5 (±9.8)
<0.001
Preoperative nursing time
13.5 (±3.6)
23.7 (±9.7)
<0.001
Postoperative nursing time
12.2 (±3.7)
12.7 (±3.4)
0.4
Postoperative nursing time
12 (±4.1)
15.8 (±6.3)
<0.001
Postoperative nursing time
12.2 (±3.9)
15 (±5.6)
<0.001
Operative time
66.2 (±29.1)
73.8 (±44.4)
0.3
Operative time
137.5 (±37.2)
146.1 (±41.1)
0.18
Operative time
117 (±68)
136 (±68.8)
<0.001
Total operation time
91.2 (±30.2)
107.4 (±46.1)
0.35
Total operation time
162.7 (±37.8)
185.4 (±39.6)
<0.001
Total operation time
143.2 (±69)
174.9 (±72,1)
<0.001
Variables mean (SD)
RARC group
Variables mean (SD)
RARN group
Dedicated nurse team (86)
No dedicated nurse team (35)
p-value
Dedicated nurse team (86)
No dedicated nurse team (35)
p-value
Preoperative nursing time
16.4 (±4.8)
29.2 (±8.9)
<0.001
Preoperative nursing time
12.6 (±2.8)
18.9 (±4.7)
<0.001
Postoperative nursing time
13 (±3.5)
15 (±4.5)
0.06
Postoperative nursing time
12.4 (±3.9)
15.3 (±5.7)
0.01
Operative time
203.4 (±68.5)
200.8 (±69.7)
0.86
Operative time
93.5 (±38.7)
93 (±42.2)
0.9
Total operation time
232.8 (±66.4)
245 (±72.6)
0.44
Total operation time
118.5 (±38.9)
127.2 (±43.1)
0.4
Note: Bold indicates significant value.
FIGURE 1
Open in figure viewerPowerPoint
Comparison of preoperative nursing time DN Team versus NoDN Team.
Conclusions
Our study suggests that the implementation of a dedicated robotic nursing team can lead to substantial reductions in overall operative time. This benefit is primarily attributed to shorter preoperative nursing times, highlighting the crucial role of the robotic nurse in optimizing the robotic surgical environment.
期刊介绍:
International Journal of Urological Nursing is an international peer-reviewed Journal for all nurses, non-specialist and specialist, who care for individuals with urological disorders. It is relevant for nurses working in a variety of settings: inpatient care, outpatient care, ambulatory care, community care, operating departments and specialist clinics. The Journal covers the whole spectrum of urological nursing skills and knowledge. It supports the publication of local issues of relevance to a wider international community to disseminate good practice.
The International Journal of Urological Nursing is clinically focused, evidence-based and welcomes contributions in the following clinical and non-clinical areas:
-General Urology-
Continence care-
Oncology-
Andrology-
Stoma care-
Paediatric urology-
Men’s health-
Uro-gynaecology-
Reconstructive surgery-
Clinical audit-
Clinical governance-
Nurse-led services-
Reflective analysis-
Education-
Management-
Research-
Leadership
The Journal welcomes original research papers, practice development papers and literature reviews. It also invites shorter papers such as case reports, critical commentary, reflective analysis and reports of audit, as well as contributions to regular sections such as the media reviews section. The International Journal of Urological Nursing supports the development of academic writing within the specialty and particularly welcomes papers from young researchers or practitioners who are seeking to build a publication profile.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


