Ahlem Achour, Jeroen Knijnenburg, Tamara Koopmann, Amir Raz, Marc Tischkowitz, Thomas D. Coates, F. Baas, C. L. Harteveld
{"title":"Moderate–severe beta-thalassemia intermedia phenotype caused by sextuplicated alpha-globin gene allele in two beta-thalassemia carriers","authors":"Ahlem Achour, Jeroen Knijnenburg, Tamara Koopmann, Amir Raz, Marc Tischkowitz, Thomas D. Coates, F. Baas, C. L. Harteveld","doi":"10.1002/ajh.27386","DOIUrl":null,"url":null,"abstract":"<p>Beta-thalassemia intermedia is caused by homo- or compound heterozygosity for beta-thalassemia variants reducing the beta-globin synthesis and encompasses a wide clinical spectrum ranging from non-transfusion dependent hemolytic anemia to occasional blood transfusion dependency. Carriers of beta-thalassemia are usually clinically asymptomatic. Only rarely beta-thalassemia carriers express symptoms of beta-thalassemia intermedia such as splenomegaly, growth retardation, and moderate to severe anemia.</p><p>In adults, HbA is composed of two alpha-globin and two beta-globin chains, which are coded for by the duplicated alpha-globin genes (<i>HBA2</i> and <i>HBA1</i>) on chromosome 16 and single beta-globin gene (<i>HBB</i>) on chromosome 11. The Major Conserved Sequences 1 to 4 (MCS1-4) regulates the expression of the alpha-genes, while the beta-Locus Control Region does the same for the beta-genes. The alpha/beta protein synthesis is balanced to a ratio of 1. Genetic defects in the globin genes may lead to a reduced or absent synthesis of alpha- or beta-globin causing alpha- or beta-thalassemia respectively. The excess of unbound alpha-globin chain forms nonfunctional unsolvable tetramers damaging the red cell membrane and is held responsible for the observed ineffective erythropoiesis in beta-thalassemia Intermedia and Major patients.<span><sup>1</sup></span> Several molecular mechanisms are held responsible of causing a beta-thalassemia intermedia phenotype in carriers. Co-inheritance of extra copies of the alpha-globin genes, causing an increasing unbalanced alpha-/beta-globin synthesis ratio is one of these mechanism.<span><sup>2</sup></span> Here we report the first alpha-cluster segmental triplication in four individuals of the same family leading to a total of eight alpha-genes. The two probands are also carrier of a known beta++-thalassemia variant (β + AATAAG ClinVar Id:15473) resulting in a moderate beta-thalassemia intermedia phenotype.</p><p>The family was referred for investigation for the first time in 2008 (father I-1, mother I-2, eldest son II-1 and proband II-2) because of a suspected beta-thalassemia trait with unexplained more severe clinical expression in proband II-2. In 2022, the family was reinvestigated after the birth of two other children, II-3 and II-4, the last showing a pronounced microcytic hypochromic anemia similar to his sister (proband II-2) (Figure 1a in Supplementary online data).</p><p>Proband II-2 was diagnosed with hypochromic microcytic anemia at 1 year of age (MCH 18.5 pg, MCV 56.8 fL, Hb 88 g/L) with mildly elevated HbA2 (3.4%) and normal ferritin (28 μg/L). She was found to be carrier of a beta+-thalassemia variant (<i>NM_000518.5(HBB):c.*113A>G</i>) inherited from her father, which however did not explain her red cell hematology. When the family was analyzed in 2022, her hematologic parameters were still low (MCH 17.9 pg, MCV 60.8 fL, Hb 90 g/L) and she had developed hepatosplenomegaly. Transfusion was started at 15 years of age.</p><p>Proband II-4 also showed a profound microcytic hypochromic anemia and hepatosplenomegaly, resembling a beta-thalassemia intermedia phenotype. He received his first transfusion at the age of 10 years. Remarkably, both probands showed very low ferritin and high zinc protoporphyrin (ZPP) in contrast to the other family members and in contrast to the analysis in 2008 when the ferritin was normal for proband II-2.</p><p>The eldest child (II-1) showed low MCV and MCH with borderline ZPP, normal ferritin levels, and a normal percentage of HbA2. The mother I-2 and her child II-3 showed normal hematology and normal HbA<sub>2</sub> levels. The father showed decreased MCV, a slightly decreased MCH, normal ferritin and marginally elevated HbA<sub>2</sub> (3.4% in 2008 and 3.2% in 2022), typical for a beta<sup>+</sup>-thalassemia carrier (Table 1 online suppmentary data).</p><p>MLPA and array analysis, performed in the probands and the parents, showed a maternally inherited interstitial triplication of the alpha-globin gene cluster on chromosome 16p13.3 (approx. 900 kb), for which the mother was approx. 25% mosaic (Figure 1b,c in Supplementary online data, Figure S1 in Supplementary material). The percentage of mosaicism was estimated using the calculated log2 ratio of Affy CytoScanHD SNP array data. Based on log2 ratio of SNPs of the gained region, the raise is approx. one-fourth in the mother, compared with the index patient (Figure S2 in Supplementary material). The triplicated DNA-segment of approx. 450 kb in length included the complete alpha-globin gene cluster, the MCS1-4 and eighteen protein-coding genes (Figure 1c in Supplementary online data). The eldest son (II-1) inherited eight alpha-genes, without the beta+-thalassemia variant of father and presented with low MCV and MCH, borderline ZPP, and normal ferritin.</p><p>To characterize the breakpoints, whole genome sequencing was performed in the proband and was suggestive of a complex rearrangement involving only the chromosome 16p 13.3 region (Figure 1A). The location of the breakpoints was also detected: the annotation of this rearrangement was seq[GRCh37] dup(16)(p13.3),trp(16)(p13.3),dup(16)(p13.3)NC_000016.9:g.pter_552829;117266_595444;552816_553125inv;113442_113601inv;133415_qter (Figure 1c in Supplementary online data).</p><p>The exact location of the breakpoints was confirmed using Sanger sequencing analysis and revealed a head-to-tail orientation as expected from WGS data (Figure S3, Table S1 in Supplementary material). This is, to our knowledge, the first report of a segmental triplication and the largest in size, containing the entire alpha-globin gene cluster and including the MCS1-4 and 18 protein-coding genes (Figure 1B). None of these genes are reported to be associated with genetic disease.</p><p>The co-inheritance of the sextuplication of the alpha-globin gene and the beta+-thalassemia variant (<i>NM_000518.5(HBB):c.*113A>G</i>) caused a moderately severe phenotype of beta-thalassemia intermedia. This confirms that the presence of eight copies of the alpha-globin gene with a mild beta-thalassemia variant actively contributes to globin chain unbalance. It is a well-known phenomenon that co-inheritance of a segmental duplication of the alpha-gene cluster and a beta+ variant causes a beta-thalassemia intermedia phenotype, which is usually not associated with transfusion dependency.<span><sup>3</sup></span> Our two patients showed severe phenotypes with low hemoglobin levels in spite of a beta<sup>++</sup> thalassemia variant; therefore, it appears that the presence of more copies of alpha-globin genes contributes to the unbalanced globin synthesis.</p><p>Both SNP array analysis and WGS revealed a maternally inherited interstitial triplication of the alpha-globin gene cluster on chromosome 16p13.3 (approx. 900 kb), for which the mother was mosaic. The 25% mosaicism was determined by SNP array analysis of DNA isolated from leucocytes and may not be representative for other tissues. WGS was indicative of a single chromosome origin showing skewed homozygosity for the SNPs in the region involved in the triplication. The complex rearrangement could be the result of a DNA replication–based mechanism of fork stalling and template switching microhomology-mediated break-induced replication (FoSTeS/MMBIR).<span><sup>4</sup></span> Moreover, Carvalho et al. proposed that complex triplications could be formed by a combination of homology-directed Break-Induced Replication (BIR) with microhomology-mediated BIR or nonhomologous end joining (NHEJ).<span><sup>5</sup></span> It seems likely that this event of in tandem triplication has occurred as a single event during early embryonic development in the mother, as she is mosaic for this rearrangement. The mosaicism involves at least the hematopoietic and the germline tissue, as she transmitted the triplication to three out of four children.</p><p>The presence of eight copies of the alpha-globin gene on its own seems not to have a discernable phenotype similar to previous cases with fewer copies of the alpha-gene where no beta-globin gene defect was present.<span><sup>6</sup></span> Indeed, the mother and the eldest son II-1 have a normal hematological phenotype. However, the presence of a relatively low MCV and MCH with normal ZPP and ferritin in the eldest child (II-1) is unexplained. Moreover, the low haptoglobin level is striking as hemolysis has not been seen in combination with the alpha thalassemia trait.</p><p>Both probands have highly elevated ZPP and low ferritin, consistent with iron deficiency. This has probably increased the phenotype severity in the two patients. Strangely, no other family member showed iron deficiency despite having the same diet. This iron deficiency could be caused by iron storage deficiency related or unrelated to their condition. To find a possible explanation for the elevated ZPP and low ferritin measured in 2022, we interpreted the WGS data of patient II-4 using Human phenotype ontology terms (Anemia HP:0001903, Iron deficiency anemia HP:0001891, Abnormality of iron homeostasis HP:0011031, Decreased total iron binding capacity HP:0033211, Decreased serum iron HP:0040303, Decreased circulating ferritin concentration HP:0012343) related to iron metabolism to eliminate any iron metabolism defect; no pathogenic variants were found in the genes related to iron metabolism associated with high ZPP and low ferritin level. Therefore, one may speculate that the eight copies of alpha-gene are interfering with iron incorporation into heme. However, low ferritin levels have not been reported in the literature in combination with alpha-gene duplication/triplication/quadruplication, and further studies are still necessary for a better understanding of this unique phenotype.</p><p>Our case confirms that the presence of eight copies of the alpha-globin gene actively contributes to the globin gene unbalance leading to a more severe beta-thalassemia intermedia phenotype in spite of a heterozygote beta<sup>++</sup> thalassemia variant. This emphasizes the importance of detecting asymptomatic carriers of these segmental triplications. Improvement in genomic technologies and the advent of the WGS allowed us to define the breakpoints, but more studies are necessary to better understand the mechanisms and effects in carriers and patients on the hematological phenotype of these complex rearrangements. WGS played a crucial role in understanding and characterizing this complex rearrangement that underline the evolving role of Next generation sequencing technologies in hemoglobinopathies.</p><p>The authors have no conflicts of interest to declare.</p><p>The authors confim that informed consent has been obtained from the involved patients and, they have given approval for this information to be published in this case report.</p>","PeriodicalId":7724,"journal":{"name":"American Journal of Hematology","volume":null,"pages":null},"PeriodicalIF":10.1000,"publicationDate":"2024-05-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.27386","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27386","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Beta-thalassemia intermedia is caused by homo- or compound heterozygosity for beta-thalassemia variants reducing the beta-globin synthesis and encompasses a wide clinical spectrum ranging from non-transfusion dependent hemolytic anemia to occasional blood transfusion dependency. Carriers of beta-thalassemia are usually clinically asymptomatic. Only rarely beta-thalassemia carriers express symptoms of beta-thalassemia intermedia such as splenomegaly, growth retardation, and moderate to severe anemia.
In adults, HbA is composed of two alpha-globin and two beta-globin chains, which are coded for by the duplicated alpha-globin genes (HBA2 and HBA1) on chromosome 16 and single beta-globin gene (HBB) on chromosome 11. The Major Conserved Sequences 1 to 4 (MCS1-4) regulates the expression of the alpha-genes, while the beta-Locus Control Region does the same for the beta-genes. The alpha/beta protein synthesis is balanced to a ratio of 1. Genetic defects in the globin genes may lead to a reduced or absent synthesis of alpha- or beta-globin causing alpha- or beta-thalassemia respectively. The excess of unbound alpha-globin chain forms nonfunctional unsolvable tetramers damaging the red cell membrane and is held responsible for the observed ineffective erythropoiesis in beta-thalassemia Intermedia and Major patients.1 Several molecular mechanisms are held responsible of causing a beta-thalassemia intermedia phenotype in carriers. Co-inheritance of extra copies of the alpha-globin genes, causing an increasing unbalanced alpha-/beta-globin synthesis ratio is one of these mechanism.2 Here we report the first alpha-cluster segmental triplication in four individuals of the same family leading to a total of eight alpha-genes. The two probands are also carrier of a known beta++-thalassemia variant (β + AATAAG ClinVar Id:15473) resulting in a moderate beta-thalassemia intermedia phenotype.
The family was referred for investigation for the first time in 2008 (father I-1, mother I-2, eldest son II-1 and proband II-2) because of a suspected beta-thalassemia trait with unexplained more severe clinical expression in proband II-2. In 2022, the family was reinvestigated after the birth of two other children, II-3 and II-4, the last showing a pronounced microcytic hypochromic anemia similar to his sister (proband II-2) (Figure 1a in Supplementary online data).
Proband II-2 was diagnosed with hypochromic microcytic anemia at 1 year of age (MCH 18.5 pg, MCV 56.8 fL, Hb 88 g/L) with mildly elevated HbA2 (3.4%) and normal ferritin (28 μg/L). She was found to be carrier of a beta+-thalassemia variant (NM_000518.5(HBB):c.*113A>G) inherited from her father, which however did not explain her red cell hematology. When the family was analyzed in 2022, her hematologic parameters were still low (MCH 17.9 pg, MCV 60.8 fL, Hb 90 g/L) and she had developed hepatosplenomegaly. Transfusion was started at 15 years of age.
Proband II-4 also showed a profound microcytic hypochromic anemia and hepatosplenomegaly, resembling a beta-thalassemia intermedia phenotype. He received his first transfusion at the age of 10 years. Remarkably, both probands showed very low ferritin and high zinc protoporphyrin (ZPP) in contrast to the other family members and in contrast to the analysis in 2008 when the ferritin was normal for proband II-2.
The eldest child (II-1) showed low MCV and MCH with borderline ZPP, normal ferritin levels, and a normal percentage of HbA2. The mother I-2 and her child II-3 showed normal hematology and normal HbA2 levels. The father showed decreased MCV, a slightly decreased MCH, normal ferritin and marginally elevated HbA2 (3.4% in 2008 and 3.2% in 2022), typical for a beta+-thalassemia carrier (Table 1 online suppmentary data).
MLPA and array analysis, performed in the probands and the parents, showed a maternally inherited interstitial triplication of the alpha-globin gene cluster on chromosome 16p13.3 (approx. 900 kb), for which the mother was approx. 25% mosaic (Figure 1b,c in Supplementary online data, Figure S1 in Supplementary material). The percentage of mosaicism was estimated using the calculated log2 ratio of Affy CytoScanHD SNP array data. Based on log2 ratio of SNPs of the gained region, the raise is approx. one-fourth in the mother, compared with the index patient (Figure S2 in Supplementary material). The triplicated DNA-segment of approx. 450 kb in length included the complete alpha-globin gene cluster, the MCS1-4 and eighteen protein-coding genes (Figure 1c in Supplementary online data). The eldest son (II-1) inherited eight alpha-genes, without the beta+-thalassemia variant of father and presented with low MCV and MCH, borderline ZPP, and normal ferritin.
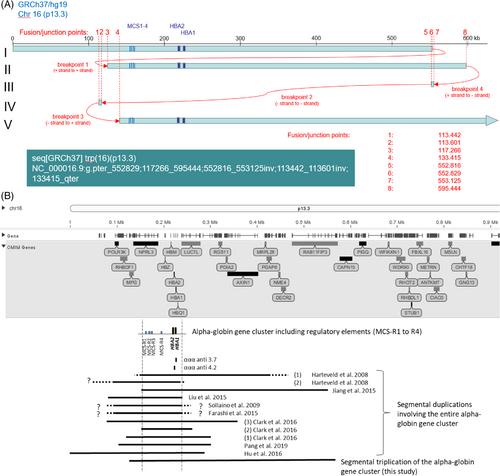
To characterize the breakpoints, whole genome sequencing was performed in the proband and was suggestive of a complex rearrangement involving only the chromosome 16p 13.3 region (Figure 1A). The location of the breakpoints was also detected: the annotation of this rearrangement was seq[GRCh37] dup(16)(p13.3),trp(16)(p13.3),dup(16)(p13.3)NC_000016.9:g.pter_552829;117266_595444;552816_553125inv;113442_113601inv;133415_qter (Figure 1c in Supplementary online data).
The exact location of the breakpoints was confirmed using Sanger sequencing analysis and revealed a head-to-tail orientation as expected from WGS data (Figure S3, Table S1 in Supplementary material). This is, to our knowledge, the first report of a segmental triplication and the largest in size, containing the entire alpha-globin gene cluster and including the MCS1-4 and 18 protein-coding genes (Figure 1B). None of these genes are reported to be associated with genetic disease.
The co-inheritance of the sextuplication of the alpha-globin gene and the beta+-thalassemia variant (NM_000518.5(HBB):c.*113A>G) caused a moderately severe phenotype of beta-thalassemia intermedia. This confirms that the presence of eight copies of the alpha-globin gene with a mild beta-thalassemia variant actively contributes to globin chain unbalance. It is a well-known phenomenon that co-inheritance of a segmental duplication of the alpha-gene cluster and a beta+ variant causes a beta-thalassemia intermedia phenotype, which is usually not associated with transfusion dependency.3 Our two patients showed severe phenotypes with low hemoglobin levels in spite of a beta++ thalassemia variant; therefore, it appears that the presence of more copies of alpha-globin genes contributes to the unbalanced globin synthesis.
Both SNP array analysis and WGS revealed a maternally inherited interstitial triplication of the alpha-globin gene cluster on chromosome 16p13.3 (approx. 900 kb), for which the mother was mosaic. The 25% mosaicism was determined by SNP array analysis of DNA isolated from leucocytes and may not be representative for other tissues. WGS was indicative of a single chromosome origin showing skewed homozygosity for the SNPs in the region involved in the triplication. The complex rearrangement could be the result of a DNA replication–based mechanism of fork stalling and template switching microhomology-mediated break-induced replication (FoSTeS/MMBIR).4 Moreover, Carvalho et al. proposed that complex triplications could be formed by a combination of homology-directed Break-Induced Replication (BIR) with microhomology-mediated BIR or nonhomologous end joining (NHEJ).5 It seems likely that this event of in tandem triplication has occurred as a single event during early embryonic development in the mother, as she is mosaic for this rearrangement. The mosaicism involves at least the hematopoietic and the germline tissue, as she transmitted the triplication to three out of four children.
The presence of eight copies of the alpha-globin gene on its own seems not to have a discernable phenotype similar to previous cases with fewer copies of the alpha-gene where no beta-globin gene defect was present.6 Indeed, the mother and the eldest son II-1 have a normal hematological phenotype. However, the presence of a relatively low MCV and MCH with normal ZPP and ferritin in the eldest child (II-1) is unexplained. Moreover, the low haptoglobin level is striking as hemolysis has not been seen in combination with the alpha thalassemia trait.
Both probands have highly elevated ZPP and low ferritin, consistent with iron deficiency. This has probably increased the phenotype severity in the two patients. Strangely, no other family member showed iron deficiency despite having the same diet. This iron deficiency could be caused by iron storage deficiency related or unrelated to their condition. To find a possible explanation for the elevated ZPP and low ferritin measured in 2022, we interpreted the WGS data of patient II-4 using Human phenotype ontology terms (Anemia HP:0001903, Iron deficiency anemia HP:0001891, Abnormality of iron homeostasis HP:0011031, Decreased total iron binding capacity HP:0033211, Decreased serum iron HP:0040303, Decreased circulating ferritin concentration HP:0012343) related to iron metabolism to eliminate any iron metabolism defect; no pathogenic variants were found in the genes related to iron metabolism associated with high ZPP and low ferritin level. Therefore, one may speculate that the eight copies of alpha-gene are interfering with iron incorporation into heme. However, low ferritin levels have not been reported in the literature in combination with alpha-gene duplication/triplication/quadruplication, and further studies are still necessary for a better understanding of this unique phenotype.
Our case confirms that the presence of eight copies of the alpha-globin gene actively contributes to the globin gene unbalance leading to a more severe beta-thalassemia intermedia phenotype in spite of a heterozygote beta++ thalassemia variant. This emphasizes the importance of detecting asymptomatic carriers of these segmental triplications. Improvement in genomic technologies and the advent of the WGS allowed us to define the breakpoints, but more studies are necessary to better understand the mechanisms and effects in carriers and patients on the hematological phenotype of these complex rearrangements. WGS played a crucial role in understanding and characterizing this complex rearrangement that underline the evolving role of Next generation sequencing technologies in hemoglobinopathies.
The authors have no conflicts of interest to declare.
The authors confim that informed consent has been obtained from the involved patients and, they have given approval for this information to be published in this case report.
期刊介绍:
The American Journal of Hematology offers extensive coverage of experimental and clinical aspects of blood diseases in humans and animal models. The journal publishes original contributions in both non-malignant and malignant hematological diseases, encompassing clinical and basic studies in areas such as hemostasis, thrombosis, immunology, blood banking, and stem cell biology. Clinical translational reports highlighting innovative therapeutic approaches for the diagnosis and treatment of hematological diseases are actively encouraged.The American Journal of Hematology features regular original laboratory and clinical research articles, brief research reports, critical reviews, images in hematology, as well as letters and correspondence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


