{"title":"Quitting smoking as a probable trigger for new-onset hypothyroidism after successful medical treatment of Graves' disease: case report.","authors":"Tamer Mohamed Elsherbiny","doi":"10.1177/20420188241256470","DOIUrl":null,"url":null,"abstract":"<p><p>Graves' disease (GD) is the most common cause of hyperthyroidism while Hashimoto or autoimmune thyroiditis is the most common cause of hypothyroidism. Spontaneous hypothyroidism may develop after successful medical treatment of GD in up to 20% of cases. This report presents a gentleman who is a known smoker and was diagnosed with GD at the age of 64 years. He was counseled about smoking cessation and started with medical treatment using carbimazole (CBZ). He was adequately controlled using medical treatment, yet he continued to smoke. After 2 years of medical treatment, CBZ was stopped due to developing hypothyroidism on the minimum dose of treatment. Celebrating the discontinuation of treatment, the patient decided to quit smoking. One month later, he was euthyroid; however, 4 months later, he developed overt hypothyroidism. He received levothyroxine replacement therapy and titrated to achieve euthyroidism and remained on levothyroxine for more than 5 years. The possibility that quitting smoking may have triggered the development of hypothyroidism was raised due to the coincidence of developing hypothyroidism only 4 months after quitting smoking. Current smoking is associated with a higher risk of developing both GD and Graves' orbitopathy. Quitting smoking is associated with a higher risk of developing new-onset thyroid autoimmunity. Quitting smoking is also associated with a sevenfold higher risk of autoimmune hypothyroidism especially in the first year of smoking cessation. Involved mechanisms may include a sudden increase in oxidative stress, a sudden increase in iodide delivery to thyroid follicles, or promoting T-helper 1-mediated autoimmune thyroiditis after quitting smoking. The present case suggests that quitting smoking may be a triggering factor for the development of hypothyroidism following successful medical treatment of GD, a phenomenon that may affect one-fifth of GD patients without previously reported triggers.</p>","PeriodicalId":22998,"journal":{"name":"Therapeutic Advances in Endocrinology and Metabolism","volume":"15 ","pages":"20420188241256470"},"PeriodicalIF":4.6000,"publicationDate":"2024-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11131390/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Endocrinology and Metabolism","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20420188241256470","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
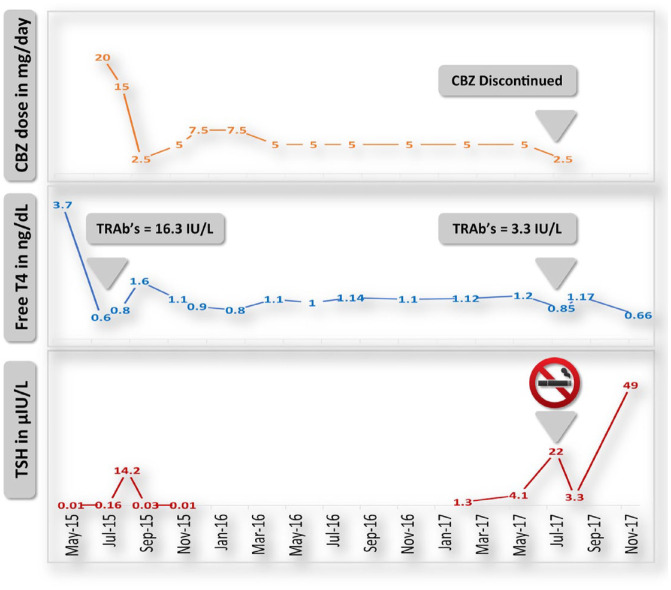
Graves' disease (GD) is the most common cause of hyperthyroidism while Hashimoto or autoimmune thyroiditis is the most common cause of hypothyroidism. Spontaneous hypothyroidism may develop after successful medical treatment of GD in up to 20% of cases. This report presents a gentleman who is a known smoker and was diagnosed with GD at the age of 64 years. He was counseled about smoking cessation and started with medical treatment using carbimazole (CBZ). He was adequately controlled using medical treatment, yet he continued to smoke. After 2 years of medical treatment, CBZ was stopped due to developing hypothyroidism on the minimum dose of treatment. Celebrating the discontinuation of treatment, the patient decided to quit smoking. One month later, he was euthyroid; however, 4 months later, he developed overt hypothyroidism. He received levothyroxine replacement therapy and titrated to achieve euthyroidism and remained on levothyroxine for more than 5 years. The possibility that quitting smoking may have triggered the development of hypothyroidism was raised due to the coincidence of developing hypothyroidism only 4 months after quitting smoking. Current smoking is associated with a higher risk of developing both GD and Graves' orbitopathy. Quitting smoking is associated with a higher risk of developing new-onset thyroid autoimmunity. Quitting smoking is also associated with a sevenfold higher risk of autoimmune hypothyroidism especially in the first year of smoking cessation. Involved mechanisms may include a sudden increase in oxidative stress, a sudden increase in iodide delivery to thyroid follicles, or promoting T-helper 1-mediated autoimmune thyroiditis after quitting smoking. The present case suggests that quitting smoking may be a triggering factor for the development of hypothyroidism following successful medical treatment of GD, a phenomenon that may affect one-fifth of GD patients without previously reported triggers.
期刊介绍:
Therapeutic Advances in Endocrinology and Metabolism delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of endocrinology and metabolism.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


