{"title":"Impact of anatomical liver resection for hepatocellular carcinoma in preventing early-phase local recurrence after surgery","authors":"Akira Shimizu, Koji Kubota, Tsuyoshi Notake, Noriyuki Kitagawa, Hitoshi Masuo, Takahiro Yoshizawa, Hiroki Sakai, Hikaru Hayashi, Shiori Yamazaki, Yuji Soejima","doi":"10.1002/jhbp.12004","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>The superiority of anatomical liver resection (AR) for localized hepatocellular carcinoma (HCC) over nonanatomical liver resection (NR) remains controversial. This study aimed to investigate the impact of AR in preventing local and early HCC recurrence.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A total of 280 patients who underwent initial liver resection for solitary HCC ≤5 cm in diameter were categorized into the AR and NR groups and compared using propensity score matching analysis.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Between the matched pairs (<i>n</i> = 87 in each group), the incidence rates of local and early (recurrence within 2 years after surgery) recurrences in the AR group were significantly lower than those in the NR group (13.8% vs. 28.7%, <i>p</i> = .025; 20.7% vs. 35.6%, <i>p</i> = .028, respectively). The overall survival in the AR group was better than that in the NR group (median: 13.4 vs. 7.6 years, <i>p</i> = .003). NR was among independent risk factors for early recurrence (odds ratio: 1.98, 95% CI: 1.1–3.6, <i>p</i> = .023) and prognostic factors for local recurrence (hazard ratio: 2.44, 95% CI: 1.4–4.4, <i>p</i> = .003).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>AR is superior in controlling local and early recurrence postoperatively for solitary HCC ≤5 cm in diameter compared with NR.</p>\n </section>\n </div>","PeriodicalId":16056,"journal":{"name":"Journal of Hepato‐Biliary‐Pancreatic Sciences","volume":"31 8","pages":"513-527"},"PeriodicalIF":3.2000,"publicationDate":"2024-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jhbp.12004","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepato‐Biliary‐Pancreatic Sciences","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jhbp.12004","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
The superiority of anatomical liver resection (AR) for localized hepatocellular carcinoma (HCC) over nonanatomical liver resection (NR) remains controversial. This study aimed to investigate the impact of AR in preventing local and early HCC recurrence.
Methods
A total of 280 patients who underwent initial liver resection for solitary HCC ≤5 cm in diameter were categorized into the AR and NR groups and compared using propensity score matching analysis.
Results
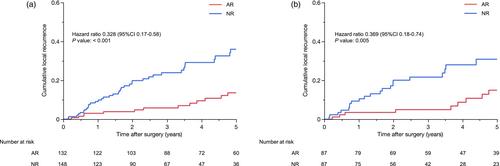
Between the matched pairs (n = 87 in each group), the incidence rates of local and early (recurrence within 2 years after surgery) recurrences in the AR group were significantly lower than those in the NR group (13.8% vs. 28.7%, p = .025; 20.7% vs. 35.6%, p = .028, respectively). The overall survival in the AR group was better than that in the NR group (median: 13.4 vs. 7.6 years, p = .003). NR was among independent risk factors for early recurrence (odds ratio: 1.98, 95% CI: 1.1–3.6, p = .023) and prognostic factors for local recurrence (hazard ratio: 2.44, 95% CI: 1.4–4.4, p = .003).
Conclusion
AR is superior in controlling local and early recurrence postoperatively for solitary HCC ≤5 cm in diameter compared with NR.
期刊介绍:
The Journal of Hepato-Biliary-Pancreatic Sciences (JHBPS) is the leading peer-reviewed journal in the field of hepato-biliary-pancreatic sciences. JHBPS publishes articles dealing with clinical research as well as translational research on all aspects of this field. Coverage includes Original Article, Review Article, Images of Interest, Rapid Communication and an announcement section. Letters to the Editor and comments on the journal’s policies or content are also included. JHBPS welcomes submissions from surgeons, physicians, endoscopists, radiologists, oncologists, and pathologists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


