Michele Lanzetti, Fabrizio Rocco Mancuso, Luca Mariano, Filippo Toaiari, Andrea Marino, Camilla Salvini, Giulia Mariotti, Emanuele Maria Cipollini
{"title":"The Horn Flap outcome in the nasal tip defect: Evaluation of postoperative scarring through patient and observer scar assessment scale score","authors":"Michele Lanzetti, Fabrizio Rocco Mancuso, Luca Mariano, Filippo Toaiari, Andrea Marino, Camilla Salvini, Giulia Mariotti, Emanuele Maria Cipollini","doi":"10.1002/jvc2.466","DOIUrl":null,"url":null,"abstract":"<p>The closure of nasal defects after oncological excision poses a great challenge, mainly because, as in this site skin is thin and rich of sebaceous glands, local flaps tend to shrink, resulting in unaesthetic trapdoor scarring.<span><sup>1, 2</sup></span> Besides grafts collected from other regions of the head do not effectively resemble skin colour and texture of this specific recipient site. The Horn Flap represents a reliable and versatile flap for reconstruction of the lateral nasal tip<span><sup>3</sup></span> and supratip. Based on a myocutaneous island flap, designed in triangular fashion reminding a rhino horn, it is achieved following a bilevel dissection (Figure 1): from one side to the depth of adipose tissue above the muscle transversalis, while on the opposite side to the depth of nasal cartilage through the muscle. The muscular pedicle, obtained through the two level undermining, provides the flap with great mobility and ensures adequate blood supply, owing to the angular artery and network of vascular anastomosis with the dorsonasal artery. To assess Horn Flap<span><sup>4</sup></span> technique effectiveness in reparation of surgical breach and its cosmetic outcomes, we collected five patients affected by basal cell carcinomas (BCC) of the nasal tip region, mean age 66.2 (SD ± 10.3), who underwent surgical reconstruction through Horn Flap in the Dermatology Surgery Department of Florence, Italy, between January 2022 and December 2022. Mean size of the defect after radicalization measured 17 mm (SD ± 0.3 mm) and all patients were treated in single stage procedure, followed by antibiotic prophylaxis. At 48 h visit flaps were vital and healed with no postoperative complications. After 1 year we performed a follow up visit aimed to scarring evaluation through the <i>Patient and Observer Scar Assessment Scale</i> (POSAS). Although it was originally developed by Draaijers<span><sup>5</sup></span> for burn scars, POSAS has shown high consistency and feasibility even when applied to postsurgical outcomes.<span><sup>6, 7</sup></span> It stands as a multidimensional tool of evaluation, entailing both observer and patient's evaluation.<span><sup>8, 9</sup></span> Every item is evaluated through a 1–10 points scale, where 1 conveys the most optimal result and 10 the worst imaginable. According to that, we submitted POSAS to our patients and to three independent dermosurgeons. The scores collected among clinicians exhibited good rates of coherency: items <i>vascularity, pigmentation, relief</i> and <i>pliability</i> achieved score 1/10 in all five cases, while item <i>thickness</i> received an average score 2.2/10, showing the three doctors shared mild concern about scar roughness. Coherently with healthcarers' point of view, the five patients delivered minimal scores (average 1.1/10) regarding <i>pain, itch, colour</i> and <i>stiffness</i>. Patients expressed slight disappointment regarding item <i>thickness</i> with average score of 1.8/10. In conclusion patients perceived their flaps as asymptomatic and almost completely resembling normal skin. Their global POSAS scores, integrated with clinicians' assessment, delivered high satisfaction regarding scar visual appearance. Doctors revealed a more critical attitude to the tactile feature of scars in two patients while, in other three cases, scars borders were not minimally detached from surrounding skin, thus not being detectable at touch. These results confirm Horn Flap is an option of the utmost value to repair surgical breach in the nasal region after BCC excision, resulting in highly acceptable aesthetical outcomes, minimal trapdoor retraction and asymptomatic scars of almost identical aspect of healthy skin (Figure 2). Moreover postsurgical evaluation through POSAS should be encouraged among healthcare professionals, as it has proven a reliable tool of assessment, comprehensive of both clinician opinion and patients' subjective attitude. From this perspective POSAS may help to individuate those patients not content with their surgical sequelae and may prompt further refining procedures like laser resurfacing or dermabrasion.</p><p><b>Michele Lanzetti</b>: Ideation of the article, drafting and revision with final approval; participation to surgical interventions as co-surgeon dermatology resident. <b>Fabrizio Rocco Mancuso</b>: Substantial contribution to ideation, drafting and revision; participation to surgical interventions as co-surgeon dermatology resident. <b>Luca Mariano</b>: Substantial contribution to ideation, drafting and revision; participation to surgical interventions as co-surgeon dermatology resident. <b>Filippo Toaiari</b>: Substantial contribution to ideation, drafting and revision; participation to surgical interventions as co-surgeon dermatology resident. <b>Andrea Marino</b>: Contribution to photographs acquisition and optimisation, drafting and final approval; participation to surgical interventions as co-surgeon dermatology resident. <b>Camilla Salvini</b>: contribution to patients treatment and follow up, ideation and final revision; main operating surgeon. <b>Giulia Mariotti</b>: contribution to patients treatment and follow up, photographs acquisition, ideation and revision; main operating surgeon. <b>Emanuele Maria Cipollini</b>: Main contribution to patients treatment and follow up, ideation and critical revision, final approval; main operating surgeon.</p><p>The authors declare no conflict of interest.</p><p>The patients in this manuscript have given written informed consent for participation in the study and the use of their deidentified, anonymized data and their case details (including photographs) for publication. Ethical approval not applicable.</p>","PeriodicalId":94325,"journal":{"name":"JEADV clinical practice","volume":"3 4","pages":"1303-1305"},"PeriodicalIF":0.0000,"publicationDate":"2024-05-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jvc2.466","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JEADV clinical practice","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jvc2.466","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
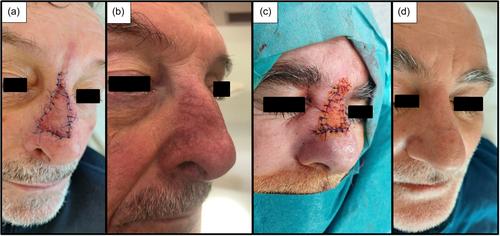
The closure of nasal defects after oncological excision poses a great challenge, mainly because, as in this site skin is thin and rich of sebaceous glands, local flaps tend to shrink, resulting in unaesthetic trapdoor scarring.1, 2 Besides grafts collected from other regions of the head do not effectively resemble skin colour and texture of this specific recipient site. The Horn Flap represents a reliable and versatile flap for reconstruction of the lateral nasal tip3 and supratip. Based on a myocutaneous island flap, designed in triangular fashion reminding a rhino horn, it is achieved following a bilevel dissection (Figure 1): from one side to the depth of adipose tissue above the muscle transversalis, while on the opposite side to the depth of nasal cartilage through the muscle. The muscular pedicle, obtained through the two level undermining, provides the flap with great mobility and ensures adequate blood supply, owing to the angular artery and network of vascular anastomosis with the dorsonasal artery. To assess Horn Flap4 technique effectiveness in reparation of surgical breach and its cosmetic outcomes, we collected five patients affected by basal cell carcinomas (BCC) of the nasal tip region, mean age 66.2 (SD ± 10.3), who underwent surgical reconstruction through Horn Flap in the Dermatology Surgery Department of Florence, Italy, between January 2022 and December 2022. Mean size of the defect after radicalization measured 17 mm (SD ± 0.3 mm) and all patients were treated in single stage procedure, followed by antibiotic prophylaxis. At 48 h visit flaps were vital and healed with no postoperative complications. After 1 year we performed a follow up visit aimed to scarring evaluation through the Patient and Observer Scar Assessment Scale (POSAS). Although it was originally developed by Draaijers5 for burn scars, POSAS has shown high consistency and feasibility even when applied to postsurgical outcomes.6, 7 It stands as a multidimensional tool of evaluation, entailing both observer and patient's evaluation.8, 9 Every item is evaluated through a 1–10 points scale, where 1 conveys the most optimal result and 10 the worst imaginable. According to that, we submitted POSAS to our patients and to three independent dermosurgeons. The scores collected among clinicians exhibited good rates of coherency: items vascularity, pigmentation, relief and pliability achieved score 1/10 in all five cases, while item thickness received an average score 2.2/10, showing the three doctors shared mild concern about scar roughness. Coherently with healthcarers' point of view, the five patients delivered minimal scores (average 1.1/10) regarding pain, itch, colour and stiffness. Patients expressed slight disappointment regarding item thickness with average score of 1.8/10. In conclusion patients perceived their flaps as asymptomatic and almost completely resembling normal skin. Their global POSAS scores, integrated with clinicians' assessment, delivered high satisfaction regarding scar visual appearance. Doctors revealed a more critical attitude to the tactile feature of scars in two patients while, in other three cases, scars borders were not minimally detached from surrounding skin, thus not being detectable at touch. These results confirm Horn Flap is an option of the utmost value to repair surgical breach in the nasal region after BCC excision, resulting in highly acceptable aesthetical outcomes, minimal trapdoor retraction and asymptomatic scars of almost identical aspect of healthy skin (Figure 2). Moreover postsurgical evaluation through POSAS should be encouraged among healthcare professionals, as it has proven a reliable tool of assessment, comprehensive of both clinician opinion and patients' subjective attitude. From this perspective POSAS may help to individuate those patients not content with their surgical sequelae and may prompt further refining procedures like laser resurfacing or dermabrasion.
Michele Lanzetti: Ideation of the article, drafting and revision with final approval; participation to surgical interventions as co-surgeon dermatology resident. Fabrizio Rocco Mancuso: Substantial contribution to ideation, drafting and revision; participation to surgical interventions as co-surgeon dermatology resident. Luca Mariano: Substantial contribution to ideation, drafting and revision; participation to surgical interventions as co-surgeon dermatology resident. Filippo Toaiari: Substantial contribution to ideation, drafting and revision; participation to surgical interventions as co-surgeon dermatology resident. Andrea Marino: Contribution to photographs acquisition and optimisation, drafting and final approval; participation to surgical interventions as co-surgeon dermatology resident. Camilla Salvini: contribution to patients treatment and follow up, ideation and final revision; main operating surgeon. Giulia Mariotti: contribution to patients treatment and follow up, photographs acquisition, ideation and revision; main operating surgeon. Emanuele Maria Cipollini: Main contribution to patients treatment and follow up, ideation and critical revision, final approval; main operating surgeon.
The authors declare no conflict of interest.
The patients in this manuscript have given written informed consent for participation in the study and the use of their deidentified, anonymized data and their case details (including photographs) for publication. Ethical approval not applicable.
Giulia Mariotti:为患者治疗和随访、照片采集、构思和修改做出贡献;主刀医生。埃马努埃莱-玛丽亚-西波利尼(Emanuele Maria Cipollini):作者声明无利益冲突。本手稿中的患者已书面知情同意参与研究,并同意将其去标识化、匿名化的数据和病例细节(包括照片)用于发表。伦理审批不适用。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


