Organization and Structures for Detection and Monitoring of CKD Across World Countries and Regions: Observational Data From a Global Survey
IF 9.4
1区 医学
Q1 UROLOGY & NEPHROLOGY
引用次数: 0
Abstract
Rationale & Objective
Established therapeutic interventions effectively mitigate the risk and progression of chronic kidney disease (CKD). Countries and regions have a compelling need for organizational structures that enable early identification of people with CKD who can benefit from these proven interventions. We report the current global status of CKD detection programs.
Study Design
A multinational cross-sectional survey.
Setting & Participants
Stakeholders, including nephrologist leaders, policymakers, and patient advocates from 167 countries, participating in the International Society of Nephrology (ISN) survey from June to September 2022.
Outcome
Structures for the detection and monitoring of CKD, including CKD surveillance systems in the form of registries, community-based detection programs, case-finding practices, and availability of measurement tools for risk identification.
Analytical Approach
Descriptive statistics.
Results
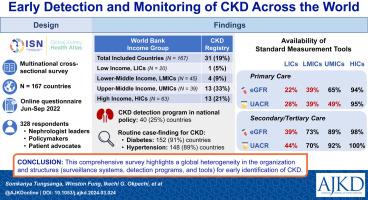
Of all participating countries, 19% (n = 31) reported CKD registries, and 25% (n = 40) reported implementing CKD detection programs as part of their national policies. There were variations in CKD detection program, with 50% (n = 20) using a reactive approach (managing cases as identified) and 50% (n = 20) actively pursuing case-finding in at-risk populations. Routine case-finding for CKD in high-risk populations was widespread, particularly for diabetes (n = 152; 91%) and hypertension (n = 148; 89%). Access to diagnostic tools, estimated glomerular filtration rate (eGFR), and urine albumin-creatinine ratio (UACR) was limited, especially in low-income (LICs) and lower-middle-income (LMICs) countries, at primary (eGFR: LICs 22%, LMICs 39%, UACR: LICs 28%, LMICs 39%) and secondary/tertiary health care levels (eGFR: LICs 39%, LMICs 73%, UACR: LICs 44%, LMICs 70%), potentially hindering CKD detection.
Limitations
A lack of detailed data prevented an in-depth analysis.
Conclusions
This comprehensive survey highlights a global heterogeneity in the organization and structures (surveillance systems and detection programs and tools) for early identification of CKD. Ongoing efforts should be geared toward bridging such disparities to optimally prevent the onset and progression of CKD and its complications.
Plain-Language Summary
Early detection and management of chronic kidney disease (CKD) is crucial to prevent progression to kidney failure. A multinational survey across 167 countries revealed disparities in CKD detection programs. Only 19% reported CKD registries, and 25% implemented detection programs as part of their national policy. Half used a reactive approach while others actively pursued case-finding in at-risk populations. Routine case-finding was common for individuals with diabetes and hypertension. However, limited access to gold standard tools such as estimated glomerular filtration rate (eGFR) and urine albumin-creatinine ratio (UACR), especially in low-income and lower-middle income countries, may hinder CKD detection. A global effort to bridge these disparities is needed to optimally prevent the onset and progression of CKD and its complications.
世界各国和各地区检测和监测慢性肾脏病的组织和结构:来自全球调查的观察数据。
理由与目标:成熟的治疗干预措施可有效降低慢性肾脏病(CKD)的风险和病情发展。各国和各地区亟需建立组织结构,以便及早发现可从这些成熟干预措施中获益的慢性肾脏病患者。我们旨在报告全球慢性肾脏病检测项目的现状:多国横断面调查:利益相关者,包括来自 167 个国家的肾脏病专家领导、政策制定者和患者权益倡导者,参与了 2022 年 6 月至 9 月的国际肾脏病学会(ISN)调查:检测和监测慢性肾脏病的结构,包括以登记册为形式的慢性肾脏病监测系统、基于社区的检测计划、病例调查实践以及用于风险识别的测量工具的可用性:分析方法:描述性统计:在所有参与国家中,19%(n=31)的国家报告了慢性肾脏病登记处,25%(n=40)的国家报告了作为国家政策一部分实施的慢性肾脏病检测计划。CKD检测计划存在差异,50%(n=20)的国家采用被动方法(发现病例后进行管理),50%(n=20)的国家在高危人群中积极开展病例调查。在高危人群中,常规的慢性肾脏病病例调查非常普遍,尤其是糖尿病(152 人;91%)和高血压(148 人;89%)。获得诊断工具--估计肾小球滤过率(eGFR)和尿白蛋白-肌酐比值(UACR)的机会有限,尤其是在低收入国家和中低收入国家的初级阶段(eGFR:eGFR:低收入国家占 22%,中低收入国家占 39%;UACR:低收入国家占 28%,中低收入国家占 39%)和二级/三级医疗保健水平(eGFR:低收入国家占 39%,中低收入国家占 73%;UACR:低收入国家占 44%,中低收入国家占 70%),这可能会阻碍 CKD 的检测。局限性:由于缺乏详细数据,无法进行深入分析:这项综合调查凸显了全球在早期识别 CKD 的组织和结构(监测系统、检测计划和工具)方面存在的差异。应继续努力缩小这些差异,以最佳方式预防慢性肾功能衰竭及其并发症的发生和发展。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

American Journal of Kidney Diseases
医学-泌尿学与肾脏学
CiteScore
20.40
自引率
2.30%
发文量
732
审稿时长
3-8 weeks
期刊介绍:
The American Journal of Kidney Diseases (AJKD), the National Kidney Foundation's official journal, is globally recognized for its leadership in clinical nephrology content. Monthly, AJKD publishes original investigations on kidney diseases, hypertension, dialysis therapies, and kidney transplantation. Rigorous peer-review, statistical scrutiny, and a structured format characterize the publication process. Each issue includes case reports unveiling new diseases and potential therapeutic strategies.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


