Pouya Motazedian, Graeme Prosperi-Porta, Benjamin Hibbert, Hawre Jalal, Marino Labinaz, Ian G Burwash, Omar Abdel-Razek, Pietro Di Santo, Trevor Simard, George Wells, Doug Coyle
{"title":"Cost-effectiveness of population screening for aortic stenosis.","authors":"Pouya Motazedian, Graeme Prosperi-Porta, Benjamin Hibbert, Hawre Jalal, Marino Labinaz, Ian G Burwash, Omar Abdel-Razek, Pietro Di Santo, Trevor Simard, George Wells, Doug Coyle","doi":"10.1093/ehjqcco/qcae043","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Aortic stenosis (AS) is a progressive disease predominantly affecting elderly patients that carries significant morbidity and mortality without aortic valve replacement, the only proven treatment. Our objective was to determine the cost-effectiveness of AS screening using transthoracic echocardiography (TTE) in a geriatric population from the perspective of the publicly funded healthcare system in Canada.</p><p><strong>Methods and results: </strong>Markov models estimating the cost-effectiveness ratio (ICER) for AS screening with a one-time TTE were developed. The model included diagnosed and undiagnosed AS health states, hospitalizations, transcatheter aortic valve replacement (TAVR), and post-TAVR health states. Primary analysis included screening at 70 and 80 years of age with intervention at symptom onset, with scenario analysis included for early intervention at the time of severe asymptomatic AS diagnosis. Monte Carlo simulation of 5000 replications was completed with a lifetime horizon and a 1.5% discount for costs and outcomes.Screening for AS at the age of 70 years was associated with an ICER of $156 722, and screening at 80 years of age was associated with an ICER of $28 005, suggesting that screening at 80 years of age is cost-effective when willingness-to-pay per QALY is $50 000. Scenario analysis with early intervention was not cost-effective, with an ICER of $142 157 at 70 years and $124 651 at 80 years.</p><p><strong>Conclusion: </strong>Screening for AS at 80 years of age with a one-time TTE, in a Canadian population, improves quality of life and is cost-effective in a publicly funded healthcare system providing, TAVR is reserved for symptomatic patients.</p>","PeriodicalId":11869,"journal":{"name":"European Heart Journal - Quality of Care and Clinical Outcomes","volume":" ","pages":"378-387"},"PeriodicalIF":4.6000,"publicationDate":"2025-06-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12187065/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal - Quality of Care and Clinical Outcomes","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ehjqcco/qcae043","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Aortic stenosis (AS) is a progressive disease predominantly affecting elderly patients that carries significant morbidity and mortality without aortic valve replacement, the only proven treatment. Our objective was to determine the cost-effectiveness of AS screening using transthoracic echocardiography (TTE) in a geriatric population from the perspective of the publicly funded healthcare system in Canada.
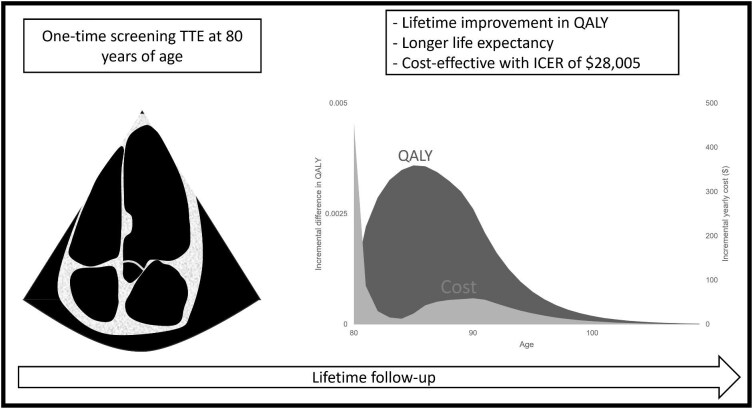
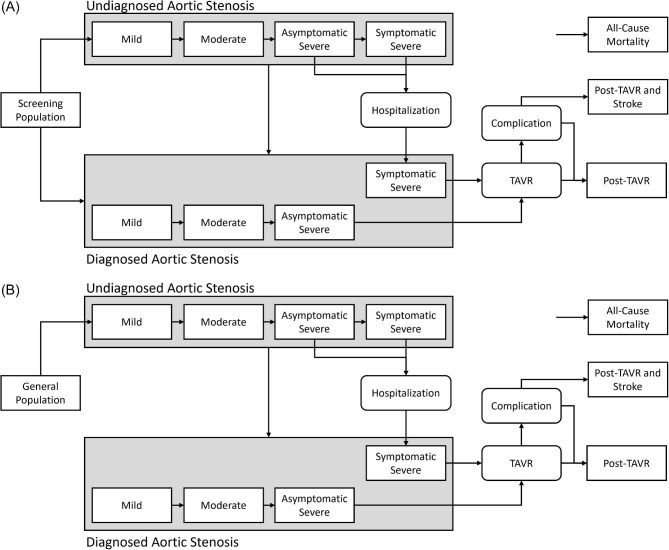
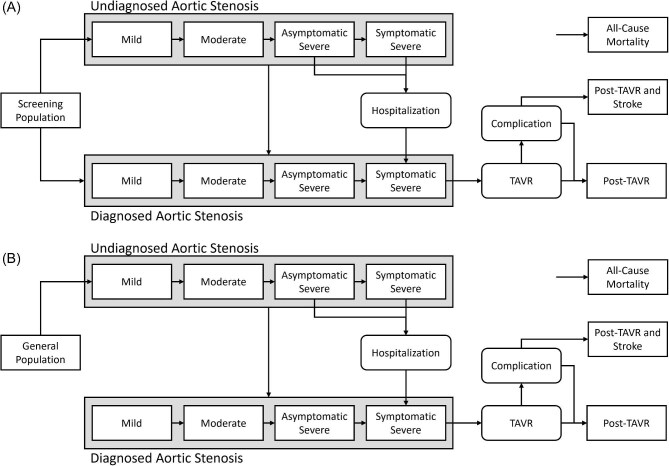
Methods and results: Markov models estimating the cost-effectiveness ratio (ICER) for AS screening with a one-time TTE were developed. The model included diagnosed and undiagnosed AS health states, hospitalizations, transcatheter aortic valve replacement (TAVR), and post-TAVR health states. Primary analysis included screening at 70 and 80 years of age with intervention at symptom onset, with scenario analysis included for early intervention at the time of severe asymptomatic AS diagnosis. Monte Carlo simulation of 5000 replications was completed with a lifetime horizon and a 1.5% discount for costs and outcomes.Screening for AS at the age of 70 years was associated with an ICER of $156 722, and screening at 80 years of age was associated with an ICER of $28 005, suggesting that screening at 80 years of age is cost-effective when willingness-to-pay per QALY is $50 000. Scenario analysis with early intervention was not cost-effective, with an ICER of $142 157 at 70 years and $124 651 at 80 years.
Conclusion: Screening for AS at 80 years of age with a one-time TTE, in a Canadian population, improves quality of life and is cost-effective in a publicly funded healthcare system providing, TAVR is reserved for symptomatic patients.
期刊介绍:
European Heart Journal - Quality of Care & Clinical Outcomes is an English language, peer-reviewed journal dedicated to publishing cardiovascular outcomes research. It serves as an official journal of the European Society of Cardiology and maintains a close alliance with the European Heart Health Institute. The journal disseminates original research and topical reviews contributed by health scientists globally, with a focus on the quality of care and its impact on cardiovascular outcomes at the hospital, national, and international levels. It provides a platform for presenting the most outstanding cardiovascular outcomes research to influence cardiovascular public health policy on a global scale. Additionally, the journal aims to motivate young investigators and foster the growth of the outcomes research community.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


