Joe Kwun Nam Chan, Corine Sau Man Wong, Catherine Zhiqian Fang, Samson Chun Hung, Heidi Ka Ying Lo, Wing Chung Chang
{"title":"Mortality risk and mood stabilizers in bipolar disorder: a propensity-score-weighted population-based cohort study in 2002-2018.","authors":"Joe Kwun Nam Chan, Corine Sau Man Wong, Catherine Zhiqian Fang, Samson Chun Hung, Heidi Ka Ying Lo, Wing Chung Chang","doi":"10.1017/S2045796024000337","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Accumulating studies have assessed mortality risk associated with mood-stabilizers, the mainstay treatment for bipolar disorder (BD). However, existing data were mostly restricted to suicide risk, focused on lithium and valproate and rarely adequately adjusted for potential confounders. This study aimed to assess comparative mortality risk with all, natural and unnatural causes between lithium, valproate and three frequently prescribed second-generation antipsychotics (SGA), with adjustment for important confounders.</p><p><strong>Methods: </strong>This population-based cohort study identified 8137 patients with first-diagnosed BD, who had exposed to lithium (<i>n</i> = 1028), valproate (<i>n</i> = 3580), olanzapine (<i>n</i> = 797), quetiapine (<i>n</i> = 1975) or risperidone (<i>n</i> = 757) between 2002 and 2018. Data were retrieved from territory-wide medical-record database of public healthcare services in Hong Kong. Propensity-score (PS)-weighting method was applied to optimize control for potential confounders including pre-existing chronic physical diseases, substance/alcohol use disorders and other psychotropic medications. PS-weighted Cox proportional-hazards regression was conducted to assess risk of all-, natural- and unnatural-cause mortality related to each mood-stabilizer, compared to lithium. Three sets of sensitivity analyses were conducted by restricting to patients with (i) length of cumulative exposure to specified mood-stabilizer ≥90 days and its medication possession ratio (MPR) ≥90%, (ii) MPR of specified mood-stabilizer ≥80% and MPR of other studied mood-stabilizers <20% and (iii) monotherapy.</p><p><strong>Results: </strong>Incidence rates of all-cause mortality per 1000 person-years were 5.9 (95% confidence interval [CI]: 4.5-7.6), 8.4 (7.4-9.5), 11.1 (8.3-14.9), 7.4 (6.0-9.2) and 12.0 (9.3-15.6) for lithium-, valproate-, olanzapine-, quetiapine- and risperidone-treated groups, respectively. BD patients treated with olanzapine (PS-weighted hazard ratio = 2.07 [95% CI: 1.33-3.22]) and risperidone (1.66 [1.08-2.55]) had significantly higher all-cause mortality rate than lithium-treated group. Olanzapine was associated with increased risk of natural-cause mortality (3.04 [1.54-6.00]) and risperidone was related to elevated risk of unnatural-cause mortality (3.33 [1.62-6.86]), relative to lithium. The association between olanzapine and increased natural-cause mortality rate was consistently affirmed in sensitivity analyses. Relationship between risperidone and elevated unnatural-cause mortality became non-significant in sensitivity analyses restricted to low MPR in other mood-stabilizers and monotherapy. Valproate- and lithium-treated groups did not show significant differences in all-, natural- or unnatural-cause mortality risk.</p><p><strong>Conclusion: </strong>Our data showed that olanzapine and risperidone were associated with higher mortality risk than lithium, and further supported the clinical guidelines recommending lithium as the first-line mood-stabilizer for BD. Future research is required to further clarify comparative mortality risk associated with individual SGA agents to facilitate risk-benefit evaluation of alternative mood-stabilizers to minimize avoidable premature mortality in BD.</p>","PeriodicalId":11787,"journal":{"name":"Epidemiology and Psychiatric Sciences","volume":"33 ","pages":"e31"},"PeriodicalIF":6.1000,"publicationDate":"2024-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11362685/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Epidemiology and Psychiatric Sciences","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1017/S2045796024000337","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Accumulating studies have assessed mortality risk associated with mood-stabilizers, the mainstay treatment for bipolar disorder (BD). However, existing data were mostly restricted to suicide risk, focused on lithium and valproate and rarely adequately adjusted for potential confounders. This study aimed to assess comparative mortality risk with all, natural and unnatural causes between lithium, valproate and three frequently prescribed second-generation antipsychotics (SGA), with adjustment for important confounders.
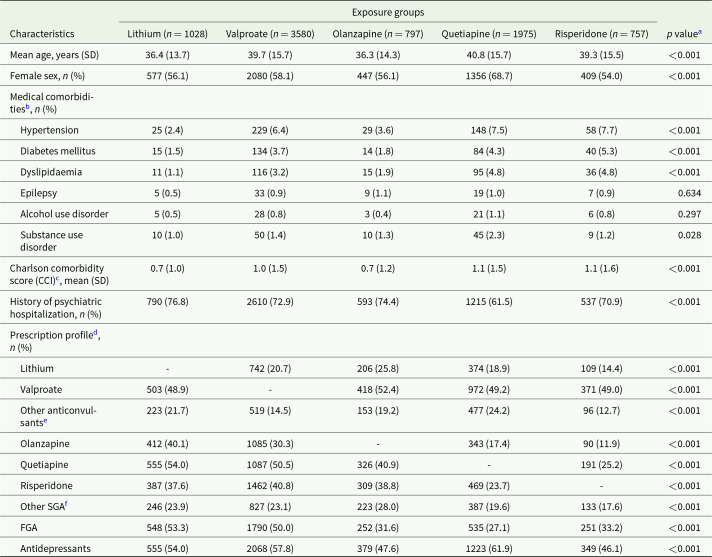
Methods: This population-based cohort study identified 8137 patients with first-diagnosed BD, who had exposed to lithium (n = 1028), valproate (n = 3580), olanzapine (n = 797), quetiapine (n = 1975) or risperidone (n = 757) between 2002 and 2018. Data were retrieved from territory-wide medical-record database of public healthcare services in Hong Kong. Propensity-score (PS)-weighting method was applied to optimize control for potential confounders including pre-existing chronic physical diseases, substance/alcohol use disorders and other psychotropic medications. PS-weighted Cox proportional-hazards regression was conducted to assess risk of all-, natural- and unnatural-cause mortality related to each mood-stabilizer, compared to lithium. Three sets of sensitivity analyses were conducted by restricting to patients with (i) length of cumulative exposure to specified mood-stabilizer ≥90 days and its medication possession ratio (MPR) ≥90%, (ii) MPR of specified mood-stabilizer ≥80% and MPR of other studied mood-stabilizers <20% and (iii) monotherapy.
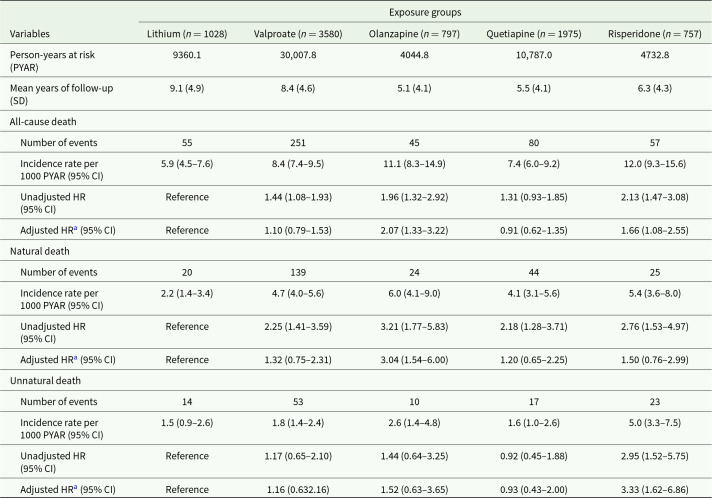
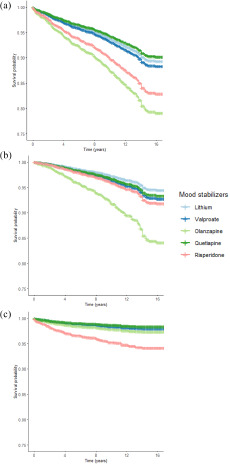
Results: Incidence rates of all-cause mortality per 1000 person-years were 5.9 (95% confidence interval [CI]: 4.5-7.6), 8.4 (7.4-9.5), 11.1 (8.3-14.9), 7.4 (6.0-9.2) and 12.0 (9.3-15.6) for lithium-, valproate-, olanzapine-, quetiapine- and risperidone-treated groups, respectively. BD patients treated with olanzapine (PS-weighted hazard ratio = 2.07 [95% CI: 1.33-3.22]) and risperidone (1.66 [1.08-2.55]) had significantly higher all-cause mortality rate than lithium-treated group. Olanzapine was associated with increased risk of natural-cause mortality (3.04 [1.54-6.00]) and risperidone was related to elevated risk of unnatural-cause mortality (3.33 [1.62-6.86]), relative to lithium. The association between olanzapine and increased natural-cause mortality rate was consistently affirmed in sensitivity analyses. Relationship between risperidone and elevated unnatural-cause mortality became non-significant in sensitivity analyses restricted to low MPR in other mood-stabilizers and monotherapy. Valproate- and lithium-treated groups did not show significant differences in all-, natural- or unnatural-cause mortality risk.
Conclusion: Our data showed that olanzapine and risperidone were associated with higher mortality risk than lithium, and further supported the clinical guidelines recommending lithium as the first-line mood-stabilizer for BD. Future research is required to further clarify comparative mortality risk associated with individual SGA agents to facilitate risk-benefit evaluation of alternative mood-stabilizers to minimize avoidable premature mortality in BD.
期刊介绍:
Epidemiology and Psychiatric Sciences is a prestigious international, peer-reviewed journal that has been publishing in Open Access format since 2020. Formerly known as Epidemiologia e Psichiatria Sociale and established in 1992 by Michele Tansella, the journal prioritizes highly relevant and innovative research articles and systematic reviews in the areas of public mental health and policy, mental health services and system research, as well as epidemiological and social psychiatry. Join us in advancing knowledge and understanding in these critical fields.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


