First Report of Two-stage Living Donor Liver Transplantation to Avoid Futility and Ensure Double Equipoise in Acute Liver Failure Complicated by Toxic Liver Syndrome
Amarnath Kadimella , Chandan K. Kedarisetty , Ravi Raya , Rajgopal M. Acharya , Smith Kadakia , Ganesh Chowhan , Gottimukkala Jayalaxmi , Mettu S. Reddy
{"title":"First Report of Two-stage Living Donor Liver Transplantation to Avoid Futility and Ensure Double Equipoise in Acute Liver Failure Complicated by Toxic Liver Syndrome","authors":"Amarnath Kadimella , Chandan K. Kedarisetty , Ravi Raya , Rajgopal M. Acharya , Smith Kadakia , Ganesh Chowhan , Gottimukkala Jayalaxmi , Mettu S. Reddy","doi":"10.1016/j.jceh.2024.101443","DOIUrl":null,"url":null,"abstract":"<div><p>Acute hepatic failure may occasionally be complicated by toxic liver syndrome. Emergency hepatectomy for stabilization followed by delayed graft implantation is a recognized strategy in such cases in the setting of deceased donor liver transplantation. Living donor liver transplantation adds additional complexity to this scenario as the donor liver is a directed donation and failure to stabilize the patient after emergency hepatectomy can lead to a futile live donor hepatectomy, hepar-divisum, or an orphan graft. We report a case where the two-stage strategy was utilized to circumvent this situation. A patient with toxic liver syndrome underwent emergency hepatectomy and was closely monitored in the operating theater. A live donor hepatectomy was started after the recipient demonstrated cardiovascular and neurological stabilization. Graft implantation was completed after an anhepatic period of 9.45 h. To our knowledge, this is the first reported instance of using the two-stage strategy in living-donor-liver-transplantation for toxic liver syndrome to prevent futile donor surgery and achieve double equipoise.</p></div>","PeriodicalId":15479,"journal":{"name":"Journal of Clinical and Experimental Hepatology","volume":"14 6","pages":"Article 101443"},"PeriodicalIF":3.3000,"publicationDate":"2024-05-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Experimental Hepatology","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0973688324001002","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
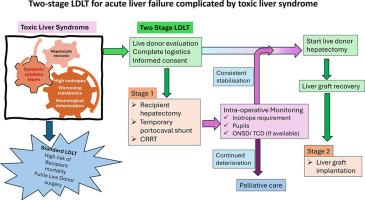
Acute hepatic failure may occasionally be complicated by toxic liver syndrome. Emergency hepatectomy for stabilization followed by delayed graft implantation is a recognized strategy in such cases in the setting of deceased donor liver transplantation. Living donor liver transplantation adds additional complexity to this scenario as the donor liver is a directed donation and failure to stabilize the patient after emergency hepatectomy can lead to a futile live donor hepatectomy, hepar-divisum, or an orphan graft. We report a case where the two-stage strategy was utilized to circumvent this situation. A patient with toxic liver syndrome underwent emergency hepatectomy and was closely monitored in the operating theater. A live donor hepatectomy was started after the recipient demonstrated cardiovascular and neurological stabilization. Graft implantation was completed after an anhepatic period of 9.45 h. To our knowledge, this is the first reported instance of using the two-stage strategy in living-donor-liver-transplantation for toxic liver syndrome to prevent futile donor surgery and achieve double equipoise.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


