Abhinav Sehgal, Arati Gangadharan, Herman A Carneiro, Graham Peigh, Jessica Charron, Graham Lohrmann, Mahmoud Elsayed, Jayson Baman, Anna Pfenniger, Kaustubha Patil, Alexandru Chicos, Rishi Arora, Susan S Kim, Albert Lin, Rod Passman, Bradley P Knight, Nishant Verma
{"title":"Safety and feasibility of intravenous sotalol loading for the prevention of ventricular arrhythmias.","authors":"Abhinav Sehgal, Arati Gangadharan, Herman A Carneiro, Graham Peigh, Jessica Charron, Graham Lohrmann, Mahmoud Elsayed, Jayson Baman, Anna Pfenniger, Kaustubha Patil, Alexandru Chicos, Rishi Arora, Susan S Kim, Albert Lin, Rod Passman, Bradley P Knight, Nishant Verma","doi":"10.1007/s10840-024-01829-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The use of intravenous (IV) sotalol loading following recent U.S. Food and Drug Administration (FDA) approval of a 1-day loading protocol has reduced the obligatory 3-day hospital stay for sotalol initiation when given orally. Several studies have recently demonstrated the safety and feasibility of IV loading for patients with atrial arrhythmias. However, there is a paucity of data on the feasibility and safety of IV sotalol loading for patients with ventricular arrhythmias. This study aims to assess the safety, feasibility, and length of stay (LOS) outcomes of IV sotalol loading for the prevention of ventricular arrhythmias.</p><p><strong>Methods: </strong>A retrospective analysis was performed of all patients undergoing IV sotalol loading and oral sotalol initiation for ventricular arrhythmias, or IV sotalol loading for atrial arrhythmias between August 2021 and December 2023 at Northwestern University. Baseline characteristics, success of sotalol initiation/loading, changes in heart rate (HR) and QT/QTc, safety, and LOS were compared between patients undergoing sotalol loading/initiation for ventricular arrhythmias (IV vs. PO) and between patients undergoing IV sotalol loading for ventricular arrhythmias vs. for atrial arrhythmias.</p><p><strong>Results: </strong>A total of 28 patients underwent sotalol loading/initiation for ventricular arrhythmias (N = 15 IV and N = 13 PO) and 41 patients underwent IV sotalol loading for atrial arrhythmias. Baseline characteristics of congestive heart failure history and left ventricular ejection fraction were worse in the ventricular arrhythmias group. There was no significant difference in the successful completion of IV sotalol loading for ventricular arrhythmias compared to oral sotalol initiation for ventricular arrhythmias or IV sotalol loading for atrial arrhythmias (86.7% vs. 92.3% vs. 90.2%, p = 0.88). There was a significant increase in ΔQTc following IV sotalol infusion for ventricular arrhythmias compared to following PO sotalol initiation for ventricular arrhythmias (46.4 ± 29.2 ms vs. 8.9 ± 32.6 ms, p = 0.004) and following IV sotalol infusion for atrial arrhythmias (46.4 ± 29.2 ms vs. 24.0 ± 25.1 ms, p = 0.018). ΔHR following IV sotalol infusion for ventricular arrhythmias was similar to ΔHR following PO sotalol initiation for ventricular arrhythmias and ΔHR following IV sotalol infusion for atrial arrhythmias (- 7.5 ± 8.7 bpm vs. - 8.5 ± 13.9 bpm vs. - 8.3 ± 13.2 bpm, p = 0.87). There were no significant differences in discontinuation for QTc prolongation (6.7% vs. 1.7% vs. 2.4%, p = 0.64) and bradycardia (13.3% vs. 7.7% vs. 9.8%, p = 0.88) between IV sotalol loading for ventricular arrhythmias, PO sotalol initiation for ventricular arrhythmias, and IV sotalol loading for atrial arrhythmias. There were no instances of hypotension, life-threatening ventricular arrhythmias, heart failure, or death. Length of stay was significantly shorter for IV sotalol loading compared to PO sotalol initiation for ventricular arrhythmias (1.1 ± 0.36 days vs. 4.2 ± 1.0 days, p < 0.0001).</p><p><strong>Conclusion: </strong>IV sotalol loading appears feasible and safe for use in ventricular arrhythmias and results in a decreased length of stay. Despite increased comorbidities and greater increase in QTc interval following IV sotalol infusion in the ventricular arrhythmias group, there were no significant differences in successful completion of loading or adverse outcomes when compared to PO sotalol initiation for ventricular arrhythmias and IV loading for atrial arrhythmias.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"1647-1655"},"PeriodicalIF":2.1000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-024-01829-4","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The use of intravenous (IV) sotalol loading following recent U.S. Food and Drug Administration (FDA) approval of a 1-day loading protocol has reduced the obligatory 3-day hospital stay for sotalol initiation when given orally. Several studies have recently demonstrated the safety and feasibility of IV loading for patients with atrial arrhythmias. However, there is a paucity of data on the feasibility and safety of IV sotalol loading for patients with ventricular arrhythmias. This study aims to assess the safety, feasibility, and length of stay (LOS) outcomes of IV sotalol loading for the prevention of ventricular arrhythmias.
Methods: A retrospective analysis was performed of all patients undergoing IV sotalol loading and oral sotalol initiation for ventricular arrhythmias, or IV sotalol loading for atrial arrhythmias between August 2021 and December 2023 at Northwestern University. Baseline characteristics, success of sotalol initiation/loading, changes in heart rate (HR) and QT/QTc, safety, and LOS were compared between patients undergoing sotalol loading/initiation for ventricular arrhythmias (IV vs. PO) and between patients undergoing IV sotalol loading for ventricular arrhythmias vs. for atrial arrhythmias.
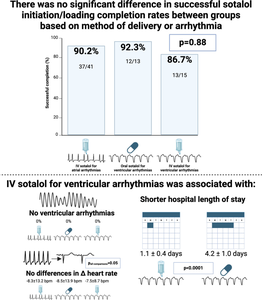
Results: A total of 28 patients underwent sotalol loading/initiation for ventricular arrhythmias (N = 15 IV and N = 13 PO) and 41 patients underwent IV sotalol loading for atrial arrhythmias. Baseline characteristics of congestive heart failure history and left ventricular ejection fraction were worse in the ventricular arrhythmias group. There was no significant difference in the successful completion of IV sotalol loading for ventricular arrhythmias compared to oral sotalol initiation for ventricular arrhythmias or IV sotalol loading for atrial arrhythmias (86.7% vs. 92.3% vs. 90.2%, p = 0.88). There was a significant increase in ΔQTc following IV sotalol infusion for ventricular arrhythmias compared to following PO sotalol initiation for ventricular arrhythmias (46.4 ± 29.2 ms vs. 8.9 ± 32.6 ms, p = 0.004) and following IV sotalol infusion for atrial arrhythmias (46.4 ± 29.2 ms vs. 24.0 ± 25.1 ms, p = 0.018). ΔHR following IV sotalol infusion for ventricular arrhythmias was similar to ΔHR following PO sotalol initiation for ventricular arrhythmias and ΔHR following IV sotalol infusion for atrial arrhythmias (- 7.5 ± 8.7 bpm vs. - 8.5 ± 13.9 bpm vs. - 8.3 ± 13.2 bpm, p = 0.87). There were no significant differences in discontinuation for QTc prolongation (6.7% vs. 1.7% vs. 2.4%, p = 0.64) and bradycardia (13.3% vs. 7.7% vs. 9.8%, p = 0.88) between IV sotalol loading for ventricular arrhythmias, PO sotalol initiation for ventricular arrhythmias, and IV sotalol loading for atrial arrhythmias. There were no instances of hypotension, life-threatening ventricular arrhythmias, heart failure, or death. Length of stay was significantly shorter for IV sotalol loading compared to PO sotalol initiation for ventricular arrhythmias (1.1 ± 0.36 days vs. 4.2 ± 1.0 days, p < 0.0001).
Conclusion: IV sotalol loading appears feasible and safe for use in ventricular arrhythmias and results in a decreased length of stay. Despite increased comorbidities and greater increase in QTc interval following IV sotalol infusion in the ventricular arrhythmias group, there were no significant differences in successful completion of loading or adverse outcomes when compared to PO sotalol initiation for ventricular arrhythmias and IV loading for atrial arrhythmias.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


