Boyu Qin, Qi Xiong, Lingli Xin, Ke Li, Weiwei Shi, Qi Song, Qiong Sun, Jiakang Shao, Jing Zhang, Xiao Zhao, Jinyu Liu, Jinliang Wang, Bo Yang
{"title":"Synergistic effect of additional anlotinib and immunotherapy as second-line or later-line treatment in pancreatic cancer: A retrospective cohort study","authors":"Boyu Qin, Qi Xiong, Lingli Xin, Ke Li, Weiwei Shi, Qi Song, Qiong Sun, Jiakang Shao, Jing Zhang, Xiao Zhao, Jinyu Liu, Jinliang Wang, Bo Yang","doi":"10.1002/cai2.123","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Pancreatic ductal adenocarcinoma (PDAC) is in urgent need of a second-line or later-line treatment strategy. We aimed to analyze the efficacy and safety of additional anlotinib, specifically anlotinib in combination with immunotherapy, in patients with PDAC who have failed first-line therapy.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Patients with pathological diagnosis of PDAC were additionally treated with anlotinib, and some patients were treated with anti-PD-1 agents at the same time, which could be retrospectively analyzed. The efficacy and safety of additional anlotinib were evaluated.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 23 patients were included. In patients treated with additional anlotinib, the overall median progression-free survival (PFS) was 1.8 months and the median overall survival (OS) was 6.3 months, regardless of anti-PD-1 agents. Among patients receiving additional anlotinib in combination with anti-PD-1 agents, median PFS and OS were 1.8 and 6.5 months, respectively. Adverse events (AEs) were observed in 16 patients (69.6%). In patients treated with additional anlotinib, the majority of AEs were grade 1–3. Univariate analysis revealed that patients with baseline red blood cell distribution width (RDW) <14% treated with additional anlotinib plus anti-PD-1 agents had significantly longer OS than patients with baseline RDW ≥14% (<i>p</i> = 0.025). Patients with additional anlotinib plus anti-PD-1 agents as second-line therapy had a longer OS than those treated as later-line therapy (<i>p</i> = 0.012). Multivariate analysis showed that baseline RDW was the only independent risk factor for OS (<i>p</i> = 0.042).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>The combination of anlotinib and immunotherapy represents an effective add-on therapy with tolerable AEs as second- or later-line therapy in patients with PDAC, particularly in patients with baseline RDW <14%.</p>\n </section>\n </div>","PeriodicalId":100212,"journal":{"name":"Cancer Innovation","volume":"3 4","pages":""},"PeriodicalIF":2.0000,"publicationDate":"2024-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cai2.123","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Innovation","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cai2.123","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Pancreatic ductal adenocarcinoma (PDAC) is in urgent need of a second-line or later-line treatment strategy. We aimed to analyze the efficacy and safety of additional anlotinib, specifically anlotinib in combination with immunotherapy, in patients with PDAC who have failed first-line therapy.
Methods
Patients with pathological diagnosis of PDAC were additionally treated with anlotinib, and some patients were treated with anti-PD-1 agents at the same time, which could be retrospectively analyzed. The efficacy and safety of additional anlotinib were evaluated.
Results
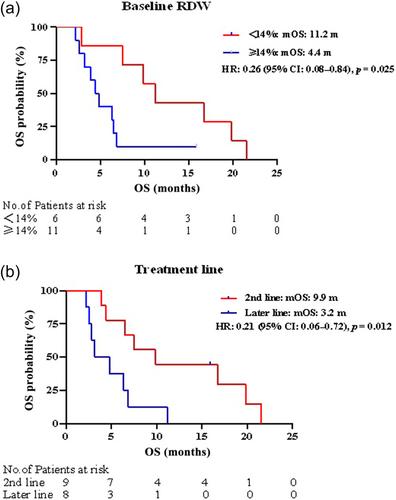
A total of 23 patients were included. In patients treated with additional anlotinib, the overall median progression-free survival (PFS) was 1.8 months and the median overall survival (OS) was 6.3 months, regardless of anti-PD-1 agents. Among patients receiving additional anlotinib in combination with anti-PD-1 agents, median PFS and OS were 1.8 and 6.5 months, respectively. Adverse events (AEs) were observed in 16 patients (69.6%). In patients treated with additional anlotinib, the majority of AEs were grade 1–3. Univariate analysis revealed that patients with baseline red blood cell distribution width (RDW) <14% treated with additional anlotinib plus anti-PD-1 agents had significantly longer OS than patients with baseline RDW ≥14% (p = 0.025). Patients with additional anlotinib plus anti-PD-1 agents as second-line therapy had a longer OS than those treated as later-line therapy (p = 0.012). Multivariate analysis showed that baseline RDW was the only independent risk factor for OS (p = 0.042).
Conclusion
The combination of anlotinib and immunotherapy represents an effective add-on therapy with tolerable AEs as second- or later-line therapy in patients with PDAC, particularly in patients with baseline RDW <14%.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


