Tom Marchant, Gareth Price, Alan McWilliam, Edward Henderson, Dónal McSweeney, Marcel van Herk, Kathryn Banfill, Matthias Schmitt, Jennifer King, Claire Barker, Corinne Faivre-Finn
{"title":"Assessment of heart-substructures auto-contouring accuracy for application in heart-sparing radiotherapy for lung cancer.","authors":"Tom Marchant, Gareth Price, Alan McWilliam, Edward Henderson, Dónal McSweeney, Marcel van Herk, Kathryn Banfill, Matthias Schmitt, Jennifer King, Claire Barker, Corinne Faivre-Finn","doi":"10.1093/bjro/tzae006","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>We validated an auto-contouring algorithm for heart substructures in lung cancer patients, aiming to establish its accuracy and reliability for radiotherapy (RT) planning. We focus on contouring an amalgamated set of subregions in the base of the heart considered to be a new organ at risk, the cardiac avoidance area (CAA), to enable maximum dose limit implementation in lung RT planning.</p><p><strong>Methods: </strong>The study validates a deep-learning model specifically adapted for auto-contouring the CAA (which includes the right atrium, aortic valve root, and proximal segments of the left and right coronary arteries). Geometric, dosimetric, quantitative, and qualitative validation measures are reported. Comparison with manual contours, including assessment of interobserver variability, and robustness testing over 198 cases are also conducted.</p><p><strong>Results: </strong>Geometric validation shows that auto-contouring performance lies within the expected range of manual observer variability despite being slightly poorer than the average of manual observers (mean surface distance for CAA of 1.6 vs 1.2 mm, dice similarity coefficient of 0.86 vs 0.88). Dosimetric validation demonstrates consistency between plans optimized using auto-contours and manual contours. Robustness testing confirms acceptable contours in all cases, with 80% rated as \"Good\" and the remaining 20% as \"Useful.\"</p><p><strong>Conclusions: </strong>The auto-contouring algorithm for heart substructures in lung cancer patients demonstrates acceptable and comparable performance to human observers.</p><p><strong>Advances in knowledge: </strong>Accurate and reliable auto-contouring results for the CAA facilitate the implementation of a maximum dose limit to this region in lung RT planning, which has now been introduced in the routine setting at our institution.</p>","PeriodicalId":72419,"journal":{"name":"BJR open","volume":"6 1","pages":"tzae006"},"PeriodicalIF":2.1000,"publicationDate":"2024-05-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11087931/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJR open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/bjro/tzae006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: We validated an auto-contouring algorithm for heart substructures in lung cancer patients, aiming to establish its accuracy and reliability for radiotherapy (RT) planning. We focus on contouring an amalgamated set of subregions in the base of the heart considered to be a new organ at risk, the cardiac avoidance area (CAA), to enable maximum dose limit implementation in lung RT planning.
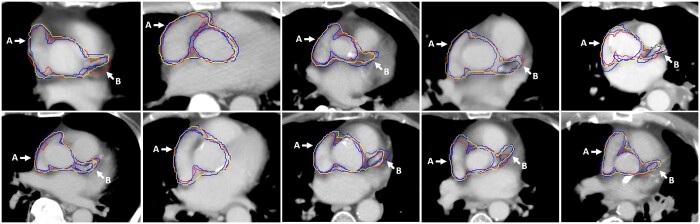
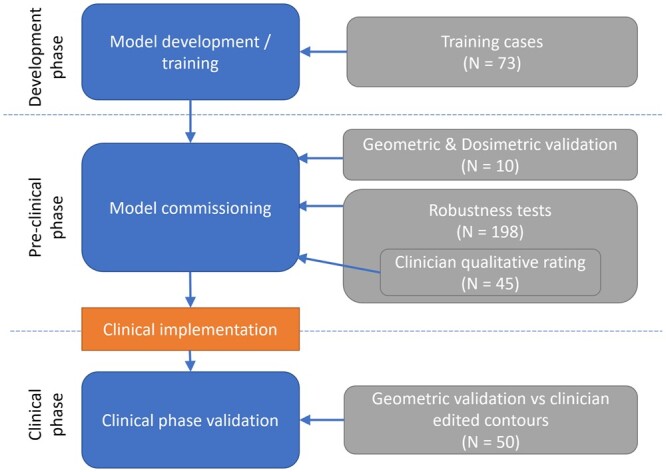
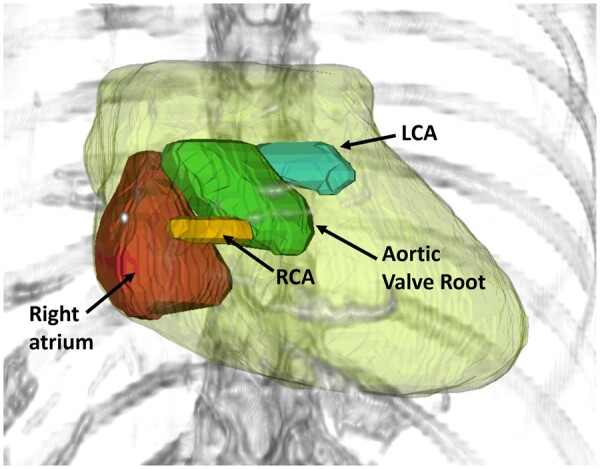
Methods: The study validates a deep-learning model specifically adapted for auto-contouring the CAA (which includes the right atrium, aortic valve root, and proximal segments of the left and right coronary arteries). Geometric, dosimetric, quantitative, and qualitative validation measures are reported. Comparison with manual contours, including assessment of interobserver variability, and robustness testing over 198 cases are also conducted.
Results: Geometric validation shows that auto-contouring performance lies within the expected range of manual observer variability despite being slightly poorer than the average of manual observers (mean surface distance for CAA of 1.6 vs 1.2 mm, dice similarity coefficient of 0.86 vs 0.88). Dosimetric validation demonstrates consistency between plans optimized using auto-contours and manual contours. Robustness testing confirms acceptable contours in all cases, with 80% rated as "Good" and the remaining 20% as "Useful."
Conclusions: The auto-contouring algorithm for heart substructures in lung cancer patients demonstrates acceptable and comparable performance to human observers.
Advances in knowledge: Accurate and reliable auto-contouring results for the CAA facilitate the implementation of a maximum dose limit to this region in lung RT planning, which has now been introduced in the routine setting at our institution.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


