Effect of neoadjuvant transarterial chemoembolization followed by resection versus upfront liver resection on the survival of single large hepatocellular carcinoma patients: A systematic review and meta-analysis.
Indah Jamtani, Toar Jean Maurice Lalisang, Wawan Mulyawan
{"title":"Effect of neoadjuvant transarterial chemoembolization followed by resection versus upfront liver resection on the survival of single large hepatocellular carcinoma patients: A systematic review and meta-analysis.","authors":"Indah Jamtani, Toar Jean Maurice Lalisang, Wawan Mulyawan","doi":"10.14701/ahbps.24-009","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgrounds/aims: </strong>The efficacy of neoadjuvant transarterial chemoembolization (N-TACE) in resectable hepatocellular carcinoma (HCC) remains open to debate. While N-TACE may reduce tumor size, its impact on long-term outcomes is inconclusive.</p><p><strong>Methods: </strong>This meta-analysis reviewed studies on N-TACE before surgical resection vs. liver resection (LR) single large hepatocellular carcinoma (SLHCC) up to March 2023 from four online databases.</p><p><strong>Results: </strong>Five studies with 1,556 patients were analyzed. No significant differences between N-TACE and LR groups were observed in 1-, 3-, or 5-year overall survival (OS) and disease-free survival (DFS). No significant differences were noted in intraoperative blood loss between groups. Subgroup analysis showed favorable 1-, 3-, and 5-year OS with combination chemotherapy N-TACE (combination group), and better 1-year OS in the LR group with single-agent chemotherapy N-TACE (single-agent group). Five-year DFS favored LR in the single-agent group, and N-TACE in the combination group.</p><p><strong>Conclusions: </strong>Managing SLHCC requires intricate considerations, and the treatment strategies for this challenging subgroup of HCC need to be improved. The influence of N-TACE on long-term survival depends on the specific chemotherapy regimen employed, and its impact on intraoperative blood loss in SLHCC appears limited.</p>","PeriodicalId":72220,"journal":{"name":"Annals of hepato-biliary-pancreatic surgery","volume":" ","pages":"325-336"},"PeriodicalIF":1.7000,"publicationDate":"2024-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11341878/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/ahbps.24-009","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/13 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Backgrounds/aims: The efficacy of neoadjuvant transarterial chemoembolization (N-TACE) in resectable hepatocellular carcinoma (HCC) remains open to debate. While N-TACE may reduce tumor size, its impact on long-term outcomes is inconclusive.
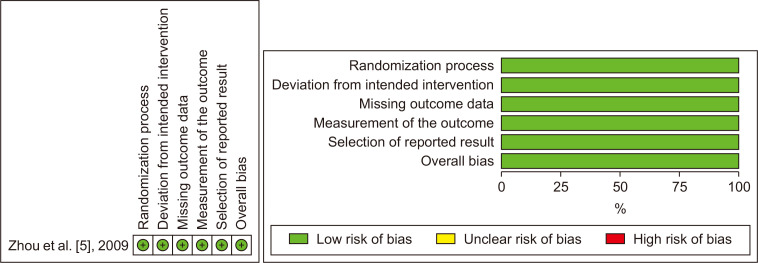
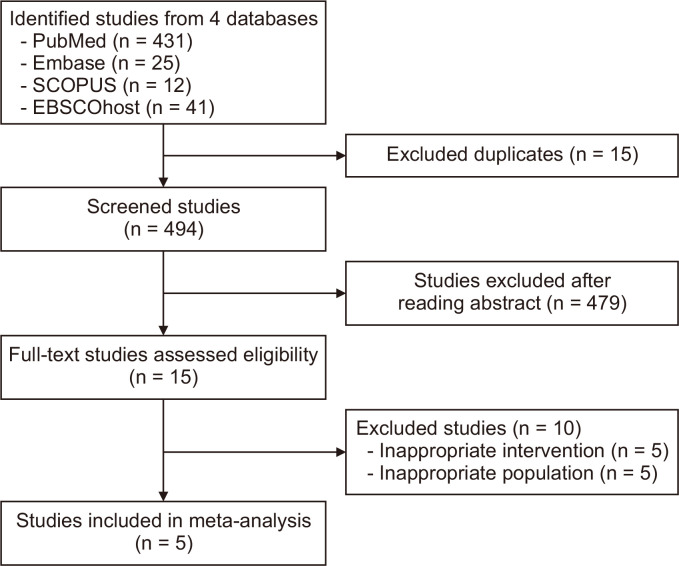
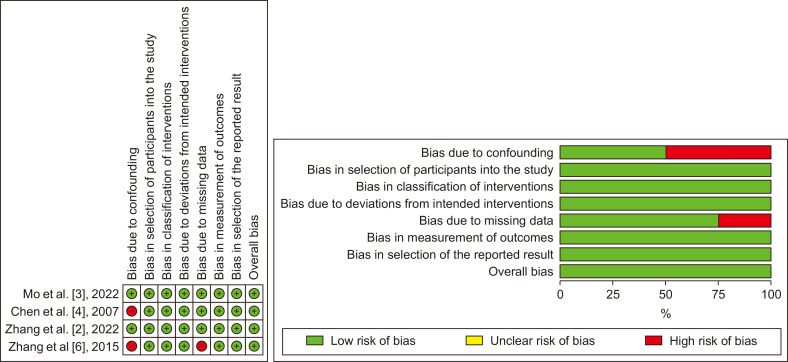
Methods: This meta-analysis reviewed studies on N-TACE before surgical resection vs. liver resection (LR) single large hepatocellular carcinoma (SLHCC) up to March 2023 from four online databases.
Results: Five studies with 1,556 patients were analyzed. No significant differences between N-TACE and LR groups were observed in 1-, 3-, or 5-year overall survival (OS) and disease-free survival (DFS). No significant differences were noted in intraoperative blood loss between groups. Subgroup analysis showed favorable 1-, 3-, and 5-year OS with combination chemotherapy N-TACE (combination group), and better 1-year OS in the LR group with single-agent chemotherapy N-TACE (single-agent group). Five-year DFS favored LR in the single-agent group, and N-TACE in the combination group.
Conclusions: Managing SLHCC requires intricate considerations, and the treatment strategies for this challenging subgroup of HCC need to be improved. The influence of N-TACE on long-term survival depends on the specific chemotherapy regimen employed, and its impact on intraoperative blood loss in SLHCC appears limited.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


