{"title":"Scoring system to predict positive peritoneal cytology in patients with resectable and borderline resectable pancreatic cancer","authors":"Tomohiro Yoshimura, Atsushi Shimizu, Yuji Kitahata, Hideki Motobayashi, Masatoshi Sato, Kyohei Matsumoto, Masaki Ueno, Shinya Hayami, Ken-ichi Okada, Manabu Kawai","doi":"10.1002/jhbp.1436","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>The aim of this study was to evaluate factors to predict positive peritoneal cytology, whcih would determine the indication for staging laparoscopy in pancreatic cancer.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A total of 430 patients that underwent pancreatectomy for resectable and borderline resectable pancreatic cancer were retrospectively reviewed.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Among 430 patients, 36 had positive cytology (8.4%). Median survival time in negative cytology was 24.7 months, compared with 15.1 months in positive cytology (<i>p</i> = .004). Factors to predict positive cytology in pancreatic cancer according to multivariate analysis were tumor location (body, tail; OR 2.66; 95% CI: 1.21–5.85; <i>p</i> = .015), tumor size ≥30 mm (OR 2.95; 95% CI: 1.35–6.47; <i>p</i> = .007) and radiographic other-organ invasion (HR 2.79; 95% CI: 1.01–7.67; <i>p</i> = .047). Patients were scored 0 to 3 corresponding with these factors. Rates of positive cytology increases in each score were: score 0: 2.9%, score 1: 6.7%, score 2: 18.3%, score 3: 36.8%.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Tumor location (body or tail), tumor size ≥30 mm, and radiographic other-organ invasions were risk factors for positive cytology in pancreatic cancer. This scoring system might be a useful indicator to perform staging laparoscopy to diagnose positive cytology.</p>\n </section>\n </div>","PeriodicalId":16056,"journal":{"name":"Journal of Hepato‐Biliary‐Pancreatic Sciences","volume":"31 7","pages":"492-502"},"PeriodicalIF":3.2000,"publicationDate":"2024-05-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepato‐Biliary‐Pancreatic Sciences","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jhbp.1436","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
The aim of this study was to evaluate factors to predict positive peritoneal cytology, whcih would determine the indication for staging laparoscopy in pancreatic cancer.
Methods
A total of 430 patients that underwent pancreatectomy for resectable and borderline resectable pancreatic cancer were retrospectively reviewed.
Results
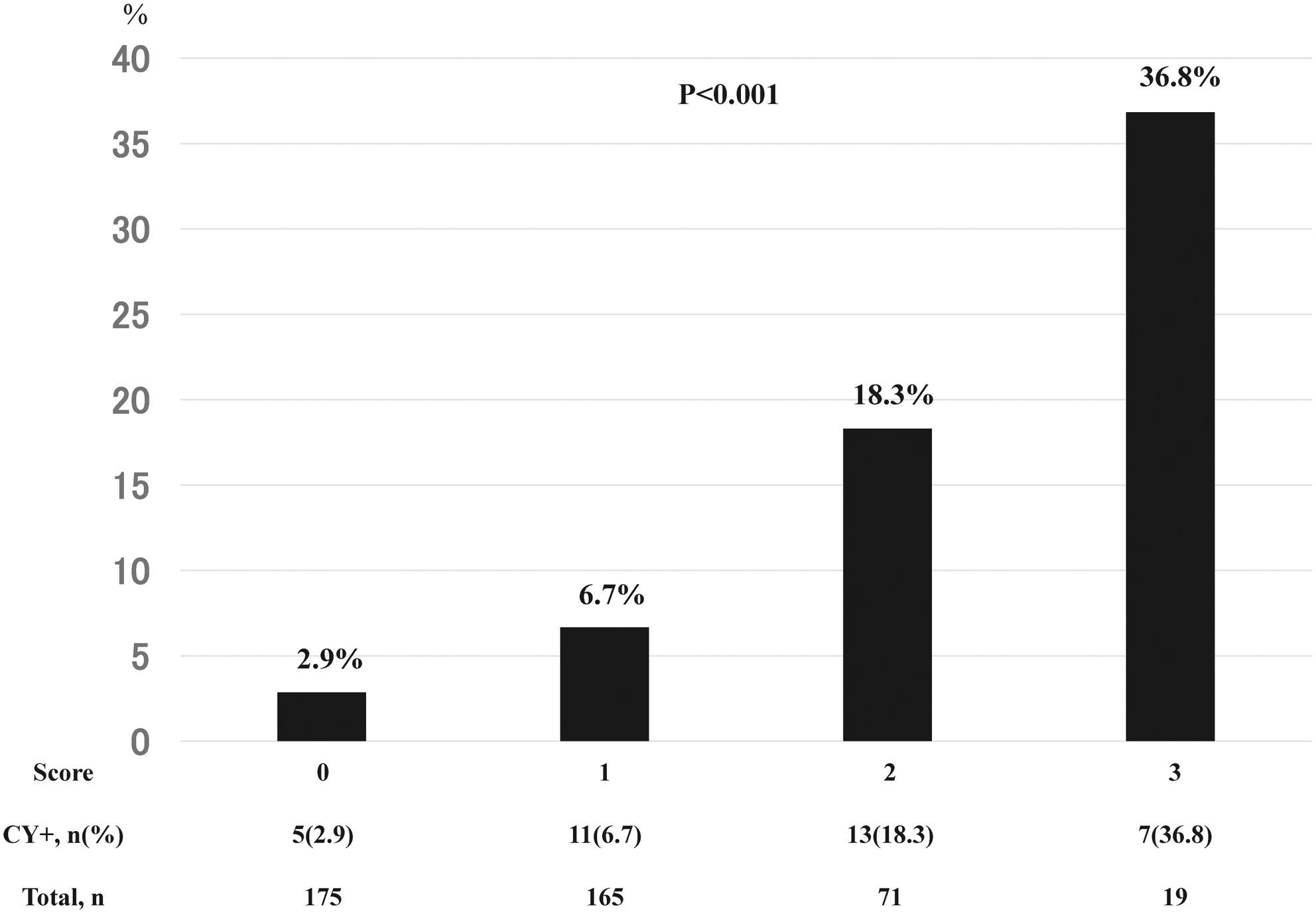
Among 430 patients, 36 had positive cytology (8.4%). Median survival time in negative cytology was 24.7 months, compared with 15.1 months in positive cytology (p = .004). Factors to predict positive cytology in pancreatic cancer according to multivariate analysis were tumor location (body, tail; OR 2.66; 95% CI: 1.21–5.85; p = .015), tumor size ≥30 mm (OR 2.95; 95% CI: 1.35–6.47; p = .007) and radiographic other-organ invasion (HR 2.79; 95% CI: 1.01–7.67; p = .047). Patients were scored 0 to 3 corresponding with these factors. Rates of positive cytology increases in each score were: score 0: 2.9%, score 1: 6.7%, score 2: 18.3%, score 3: 36.8%.
Conclusions
Tumor location (body or tail), tumor size ≥30 mm, and radiographic other-organ invasions were risk factors for positive cytology in pancreatic cancer. This scoring system might be a useful indicator to perform staging laparoscopy to diagnose positive cytology.
期刊介绍:
The Journal of Hepato-Biliary-Pancreatic Sciences (JHBPS) is the leading peer-reviewed journal in the field of hepato-biliary-pancreatic sciences. JHBPS publishes articles dealing with clinical research as well as translational research on all aspects of this field. Coverage includes Original Article, Review Article, Images of Interest, Rapid Communication and an announcement section. Letters to the Editor and comments on the journal’s policies or content are also included. JHBPS welcomes submissions from surgeons, physicians, endoscopists, radiologists, oncologists, and pathologists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


