{"title":"Should an Incidental Meckel Diverticulum Be Resected? A Systematic Review.","authors":"Vipul D Yagnik, Pankaj Garg, Sushil Dawka","doi":"10.2147/CEG.S460053","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Meckel Diverticulum [MD), a common congenital anomaly of the gastrointestinal tract, poses a dilemma when incidentally encountered during surgery. Despite historical descriptions and known complications of symptomatic MD, the decision to resect an incidental MD (IMD) lacks clear guidelines. This study aims to assess whether resecting IMDs is justified by synthesizing evidence from studies published between 2000 and 2023. Factors influencing this decision, such as demographic risks, surgical advancements and complications, are systematically examined.</p><p><strong>Methods and material: </strong>Following the PRISMA 2020 guidelines, this review incorporates 42 eligible studies with data on outcomes of asymptomatic MD management. Studies, both favoring and opposing resection, were analyzed.</p><p><strong>Results: </strong>Considering complications, malignancy potential, and operative safety, the risk-benefit analysis presents a nuanced picture. Some authors propose conditional resection based on specific criteria, emphasizing patient-specific factors. Of 2934 cases analyzed for short- and long-term complications, the morbidity rate was 5.69%. Of 571 cases where mortality data were available, all 5 fatalities were attributed to the primary disease rather than IMD resection.</p><p><strong>Conclusion: </strong>The sporadic, unpredictable presentation of IMD and the variability of both the primary disease and the patient make formulation of definitive guidelines challenging. The non-uniformity of complications reporting underscores the need for standardized categorization. While the balance of evidence leans towards resection of IMDs, this study acknowledges the individualized nature of this decision. Increased safety in surgery and anesthesia, along with better understanding and management of complications favor a judicious preference for resection, while taking into account patient characteristics and the primary disease.</p>","PeriodicalId":10208,"journal":{"name":"Clinical and Experimental Gastroenterology","volume":"17 ","pages":"147-155"},"PeriodicalIF":2.3000,"publicationDate":"2024-05-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11088382/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEG.S460053","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Meckel Diverticulum [MD), a common congenital anomaly of the gastrointestinal tract, poses a dilemma when incidentally encountered during surgery. Despite historical descriptions and known complications of symptomatic MD, the decision to resect an incidental MD (IMD) lacks clear guidelines. This study aims to assess whether resecting IMDs is justified by synthesizing evidence from studies published between 2000 and 2023. Factors influencing this decision, such as demographic risks, surgical advancements and complications, are systematically examined.
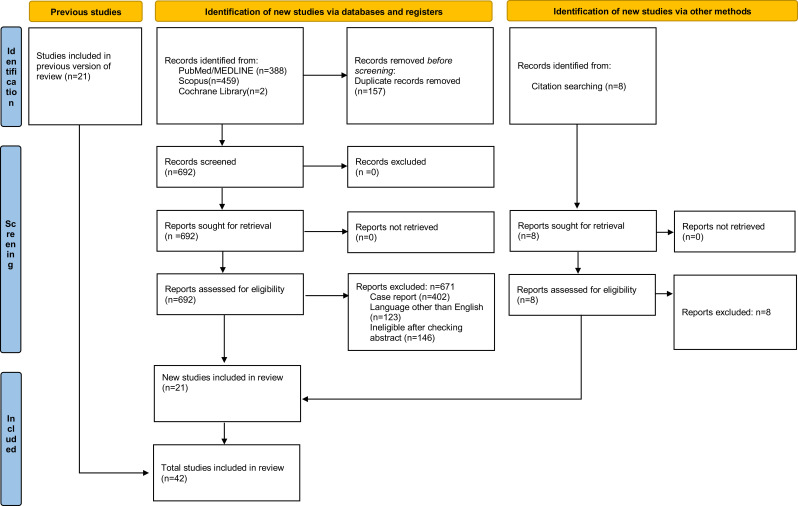
Methods and material: Following the PRISMA 2020 guidelines, this review incorporates 42 eligible studies with data on outcomes of asymptomatic MD management. Studies, both favoring and opposing resection, were analyzed.
Results: Considering complications, malignancy potential, and operative safety, the risk-benefit analysis presents a nuanced picture. Some authors propose conditional resection based on specific criteria, emphasizing patient-specific factors. Of 2934 cases analyzed for short- and long-term complications, the morbidity rate was 5.69%. Of 571 cases where mortality data were available, all 5 fatalities were attributed to the primary disease rather than IMD resection.
Conclusion: The sporadic, unpredictable presentation of IMD and the variability of both the primary disease and the patient make formulation of definitive guidelines challenging. The non-uniformity of complications reporting underscores the need for standardized categorization. While the balance of evidence leans towards resection of IMDs, this study acknowledges the individualized nature of this decision. Increased safety in surgery and anesthesia, along with better understanding and management of complications favor a judicious preference for resection, while taking into account patient characteristics and the primary disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


