{"title":"Transitioning to peritoneal dialysis: it does not matter where you come from.","authors":"Diogo Francisco, Andreia Carnevale, Gonçalo Ávila, Ana Rita Calça, Patrícia Matias, Patrícia Branco","doi":"10.1590/2175-8239-JBN-2023-0139en","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Patients with end-stage renal disease (ESRD) frequently change renal replacement (RRT) therapy modality due to medical or social reasons. We aimed to evaluate the outcomes of patients under peritoneal dialysis (PD) according to the preceding RRT modality.</p><p><strong>Methods: </strong>We conducted a retrospective observational single-center study in prevalent PD patients from January 1, 2010, to December 31, 2017, who were followed for 60 months or until they dropped out of PD. Patients were divided into three groups according to the preceding RRT: prior hemodialysis (HD), failed kidney transplant (KT), and PD-first.</p><p><strong>Results: </strong>Among 152 patients, 115 were PD-first, 22 transitioned from HD, and 15 from a failing KT. There was a tendency for ultrafiltration failure to occur more in patients transitioning from HD (27.3% vs. 9.6% vs. 6.7%, p = 0.07). Residual renal function was better preserved in the group with no prior RRT (p < 0.001). A tendency towards a higher annual rate of peritonitis was observed in the prior KT group (0.70 peritonitis/year per patient vs. 0.10 vs. 0.21, p = 0.065). Thirteen patients (8.6%) had a major cardiovascular event, 5 of those had been transferred from a failing KT (p = 0.004). There were no differences between PD-first, prior KT, and prior HD in terms of death and technique survival (p = 0.195 and p = 0.917, respectively) and PD efficacy was adequate in all groups.</p><p><strong>Conclusions: </strong>PD is a suitable option for ESRD patients regardless of the previous RRT and should be offered to patients according to their clinical and social status and preferences.</p>","PeriodicalId":14724,"journal":{"name":"Jornal brasileiro de nefrologia : 'orgao oficial de Sociedades Brasileira e Latino-Americana de Nefrologia","volume":"46 3","pages":"e20230139"},"PeriodicalIF":1.3000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11287956/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Jornal brasileiro de nefrologia : 'orgao oficial de Sociedades Brasileira e Latino-Americana de Nefrologia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1590/2175-8239-JBN-2023-0139en","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Patients with end-stage renal disease (ESRD) frequently change renal replacement (RRT) therapy modality due to medical or social reasons. We aimed to evaluate the outcomes of patients under peritoneal dialysis (PD) according to the preceding RRT modality.
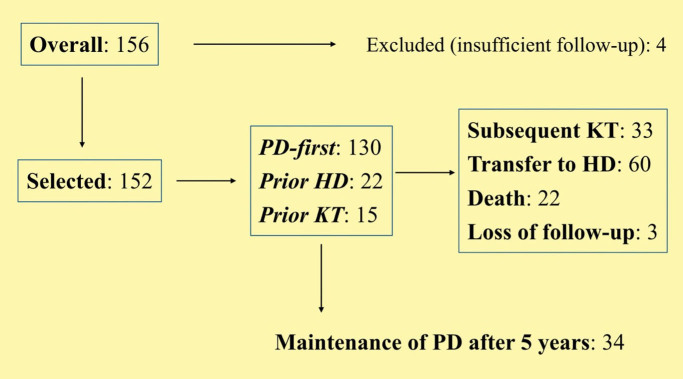
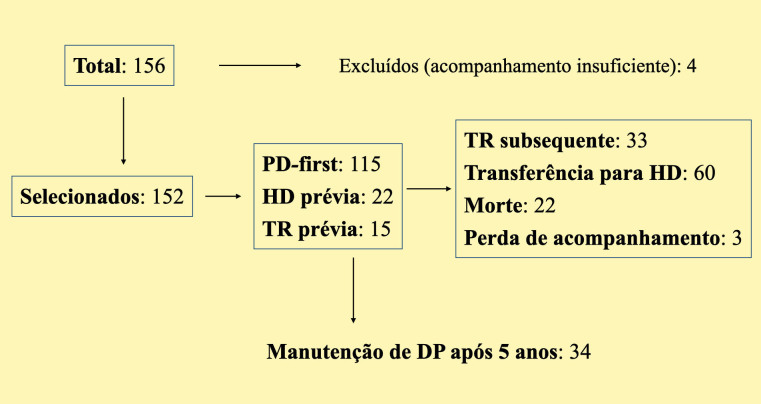
Methods: We conducted a retrospective observational single-center study in prevalent PD patients from January 1, 2010, to December 31, 2017, who were followed for 60 months or until they dropped out of PD. Patients were divided into three groups according to the preceding RRT: prior hemodialysis (HD), failed kidney transplant (KT), and PD-first.
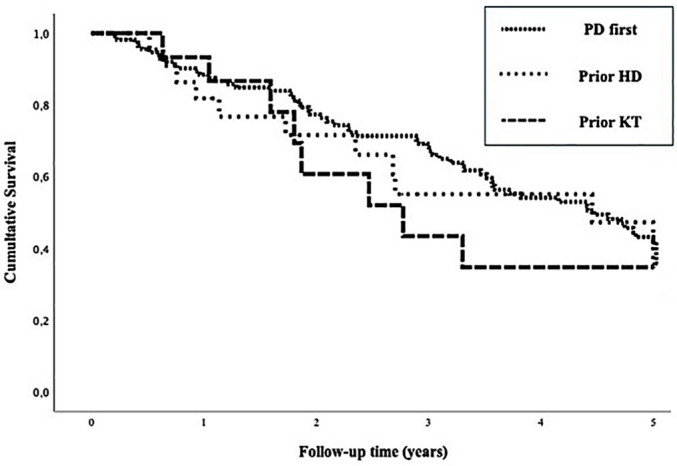
Results: Among 152 patients, 115 were PD-first, 22 transitioned from HD, and 15 from a failing KT. There was a tendency for ultrafiltration failure to occur more in patients transitioning from HD (27.3% vs. 9.6% vs. 6.7%, p = 0.07). Residual renal function was better preserved in the group with no prior RRT (p < 0.001). A tendency towards a higher annual rate of peritonitis was observed in the prior KT group (0.70 peritonitis/year per patient vs. 0.10 vs. 0.21, p = 0.065). Thirteen patients (8.6%) had a major cardiovascular event, 5 of those had been transferred from a failing KT (p = 0.004). There were no differences between PD-first, prior KT, and prior HD in terms of death and technique survival (p = 0.195 and p = 0.917, respectively) and PD efficacy was adequate in all groups.
Conclusions: PD is a suitable option for ESRD patients regardless of the previous RRT and should be offered to patients according to their clinical and social status and preferences.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


