{"title":"Diagnostic Indicators of ECG for Coronary Slow Flow Phenomenon; a Systematic Review and Meta-Analysis.","authors":"MohammadHossein MozafaryBazargany, Parham Samimisedeh, Niloofar Gholami, Elmira Jafari Afshar, Amirhossein Memari, Shahrooz Yazdani, Hadith Rastad","doi":"10.22037/aaem.v12i1.2202","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Currently, epicardial coronary angiography is still the only diagnostic tool for Coronary Slow Flow Phenomenon (CSFP). This study aimed to systematically review studies that compared Electrocardiogram (ECG) findings between patients with and without CSFP.</p><p><strong>Methods: </strong>Using relevant key terms, we systematically searched MEDLINE, Scopus, Embase, and Web of Science to find relevant studies up to February 5<sup>th</sup>, 2023. Effect sizes in each study were calculated as mean differences and crude odds ratio; then, random-effect models using inverse variance and Mantel-Haenszel methods were used to pool standardized mean differences (SMD) and crude odds ratios, respectively.</p><p><strong>Results: </strong>Thirty-two eligible articles with a total sample size of 3,937 patients (2,069 with CSFP) were included. CSFP patients had higher P-wave maximum (Pmax) (SMD: 1.02 (95% confidence interval (CI): 0.29 - 1.76); p=0.006) and P-dispersion (Pd) (SMD: 1.63 (95% CI: 0.99 - 2.27); p<0.001) compared to the control group. CSFP group also showed significantly longer QT wave maximum duration (SMD: 0.69 (95% CI: 0.33 - 1.06); p<0.001), uncorrected QTd (SMD: 1.89(95% CI: 0.67 - 3.11); p=0.002), and corrected dispersion (QTcd) (SMD: 1.63 (95% CI: 1.09 - 2.17), p<0.001). The frontal QRS-T angle was significantly higher in the CSFP group in comparison with the control group (SMD: 1.18 (95% CI: 0.31 - 2.04; p=0.007). While CSFP patients had a significantly higher T-peak to T-end (Tp-e) (SMD:1.71 (95% CI: 0.91, 2.52), p<0.001), no significant difference was noted between groups in terms of Tp-e to QT (p=0.16) and corrected QT ratios (p=0.07).</p><p><strong>Conclusion: </strong>Our findings suggest several ECG parameters, such as P max, Pd, QT, QTc, QTd, QTcd, Tp-e, and frontal QRS-T angle, may be prolonged in CSFP patients, and they could be employed as diagnostic indicators of CSFP before angiography.</p>","PeriodicalId":8146,"journal":{"name":"Archives of Academic Emergency Medicine","volume":"12 1","pages":"e34"},"PeriodicalIF":2.0000,"publicationDate":"2024-03-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11077394/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Academic Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22037/aaem.v12i1.2202","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Currently, epicardial coronary angiography is still the only diagnostic tool for Coronary Slow Flow Phenomenon (CSFP). This study aimed to systematically review studies that compared Electrocardiogram (ECG) findings between patients with and without CSFP.
Methods: Using relevant key terms, we systematically searched MEDLINE, Scopus, Embase, and Web of Science to find relevant studies up to February 5th, 2023. Effect sizes in each study were calculated as mean differences and crude odds ratio; then, random-effect models using inverse variance and Mantel-Haenszel methods were used to pool standardized mean differences (SMD) and crude odds ratios, respectively.
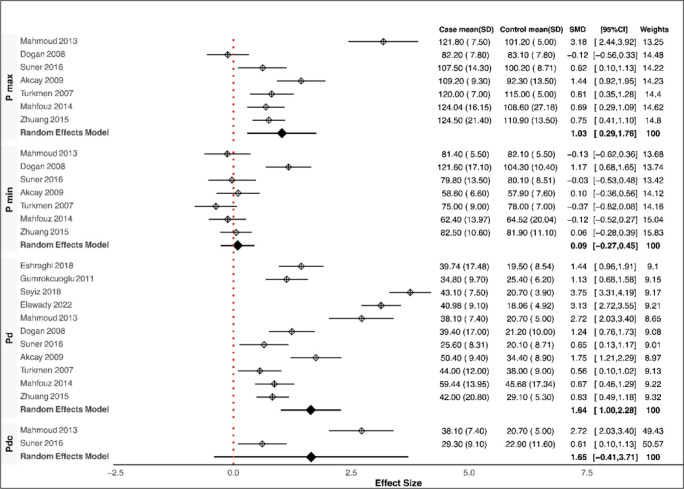
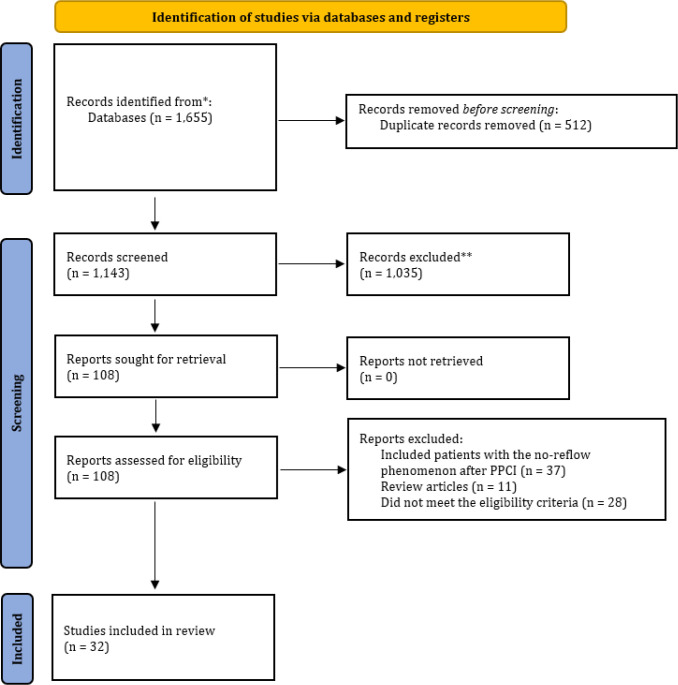
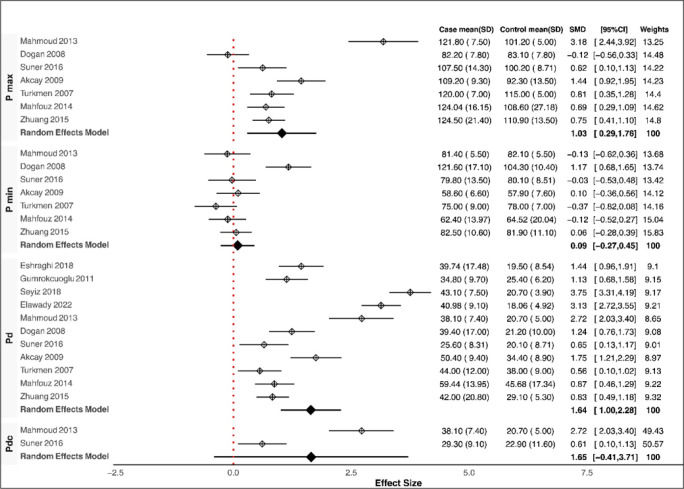
Results: Thirty-two eligible articles with a total sample size of 3,937 patients (2,069 with CSFP) were included. CSFP patients had higher P-wave maximum (Pmax) (SMD: 1.02 (95% confidence interval (CI): 0.29 - 1.76); p=0.006) and P-dispersion (Pd) (SMD: 1.63 (95% CI: 0.99 - 2.27); p<0.001) compared to the control group. CSFP group also showed significantly longer QT wave maximum duration (SMD: 0.69 (95% CI: 0.33 - 1.06); p<0.001), uncorrected QTd (SMD: 1.89(95% CI: 0.67 - 3.11); p=0.002), and corrected dispersion (QTcd) (SMD: 1.63 (95% CI: 1.09 - 2.17), p<0.001). The frontal QRS-T angle was significantly higher in the CSFP group in comparison with the control group (SMD: 1.18 (95% CI: 0.31 - 2.04; p=0.007). While CSFP patients had a significantly higher T-peak to T-end (Tp-e) (SMD:1.71 (95% CI: 0.91, 2.52), p<0.001), no significant difference was noted between groups in terms of Tp-e to QT (p=0.16) and corrected QT ratios (p=0.07).
Conclusion: Our findings suggest several ECG parameters, such as P max, Pd, QT, QTc, QTd, QTcd, Tp-e, and frontal QRS-T angle, may be prolonged in CSFP patients, and they could be employed as diagnostic indicators of CSFP before angiography.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


