Comparative Evaluation of Caudal Epidural Method to Ultrasound-Guided S1 Transforamen Block in Patient's Lumbar Discectomy with Failed Back Syndrome Symptoms: A Double-Blind Clinical Trial.
{"title":"Comparative Evaluation of Caudal Epidural Method to Ultrasound-Guided S1 Transforamen Block in Patient's Lumbar Discectomy with Failed Back Syndrome Symptoms: A Double-Blind Clinical Trial.","authors":"Masoud Hashemi, Artadokht Khoshooei, Alireza Amanollahi, Sogol Asgari","doi":"10.5812/aapm-137325","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Post-lumbar surgery syndrome (PLSS) refers to persistent or recurrent pain following spinal surgery with an unknown cause. It is commonly associated with epidural fibrosis (EF). Some studies suggest that epidural steroid injection (ESI) can effectively alleviate pain in PLSS, particularly when targeting the S1 nerve root using S1 transforaminal epidural steroid injection (S1-TFESI). A key factor in a successful block is accurately visualizing the first dorsal sacral foramen, and the needle's destination is the dorsal S1 foramen. Although S1-TFESI is often performed under fluoroscopy through the transforaminal route, an alternative to reduce radiation exposure is ultrasound guidance. This study aimed to compare the efficacy of ultrasound-guided caudal epidural steroid injection (CESI) and S1-TFESI in PLSS patients.</p><p><strong>Methods: </strong>A randomized double-blinded clinical trial was conducted involving 52 PLSS patients who were randomly assigned to either the CESI group or the S1-TFESI group. The patients were positioned prone. A linear transducer with a curve at a low frequency (2 - 5 MHz) was used to visualize the area. An aseptically prepared puncture site was used to insert a 2- to 5-MHz curved ultrasound probe with an ultrasound gel to identify the articular processes of the lower lumbar vertebrae and the posterior sacral surface. The probe was then positioned longitudinally to the para-sacral area, about 2 cm lateral to the midline. The articular process represented the L5/S1 level at the farthest caudal side, and the S1 posterior sacral foramen was represented by the concavity at the posterior sacral surface that was somewhat caudal. The probe was angled caudally to provide enough room for the needle to enter the S1 foramen. The injection site for the needle tip was the S1 foramen. A combination of triamcinolone (40 mg, 1 mL), normal saline (2 mL), and ropivacaine (0.2%) was administered. For TFS1 ESI, 5 mL of the combination was used. For CESI, the sacral hiatus was palpated in the prone position, and a linear high-frequency transducer was placed transversely to obtain a transverse view of the sacral hiatus. A combination of triamcinolone 40 mg and ropivacaine (0.2%) totaling 10 mL was employed. The Numerical Rating Scale (NRS) and Oswestry Disability Index (ODI) were used to assess patients' preoperative and postoperative conditions, and adverse events were recorded. Follow-up was conducted one week and one month after the procedures.</p><p><strong>Results: </strong>In both groups, NRS and ODI scores decreased at different time points after treatment, compared to baseline (P < 0.001). The CESI group had lower median ODI scores after one week and one month, although this difference did not reach statistical significance (P = 0.334). Despite similar baseline NRS ratings, the CESI group had statistically significantly lower mean NRS scores at one week and one month (P < 0.001).</p><p><strong>Conclusions: </strong>The current study demonstrated that both CESI and TFESI treatments for PLSS following lumbar discectomy are effective and safe. These procedures can alleviate pain and reduce disability. Although the success rates of the two procedures are comparable, CESI appears to be more successful in reducing pain at the one-week and one-month follow-up.</p>","PeriodicalId":7841,"journal":{"name":"Anesthesiology and Pain Medicine","volume":"13 6","pages":"e137325"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11078231/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesiology and Pain Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5812/aapm-137325","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Post-lumbar surgery syndrome (PLSS) refers to persistent or recurrent pain following spinal surgery with an unknown cause. It is commonly associated with epidural fibrosis (EF). Some studies suggest that epidural steroid injection (ESI) can effectively alleviate pain in PLSS, particularly when targeting the S1 nerve root using S1 transforaminal epidural steroid injection (S1-TFESI). A key factor in a successful block is accurately visualizing the first dorsal sacral foramen, and the needle's destination is the dorsal S1 foramen. Although S1-TFESI is often performed under fluoroscopy through the transforaminal route, an alternative to reduce radiation exposure is ultrasound guidance. This study aimed to compare the efficacy of ultrasound-guided caudal epidural steroid injection (CESI) and S1-TFESI in PLSS patients.
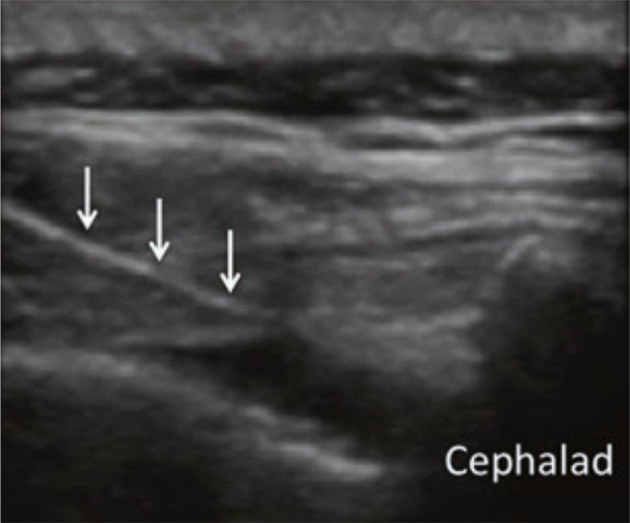
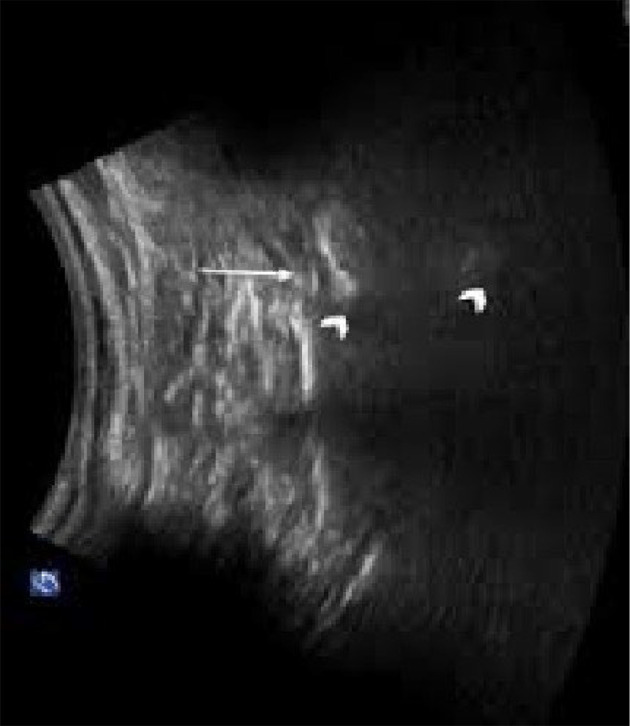
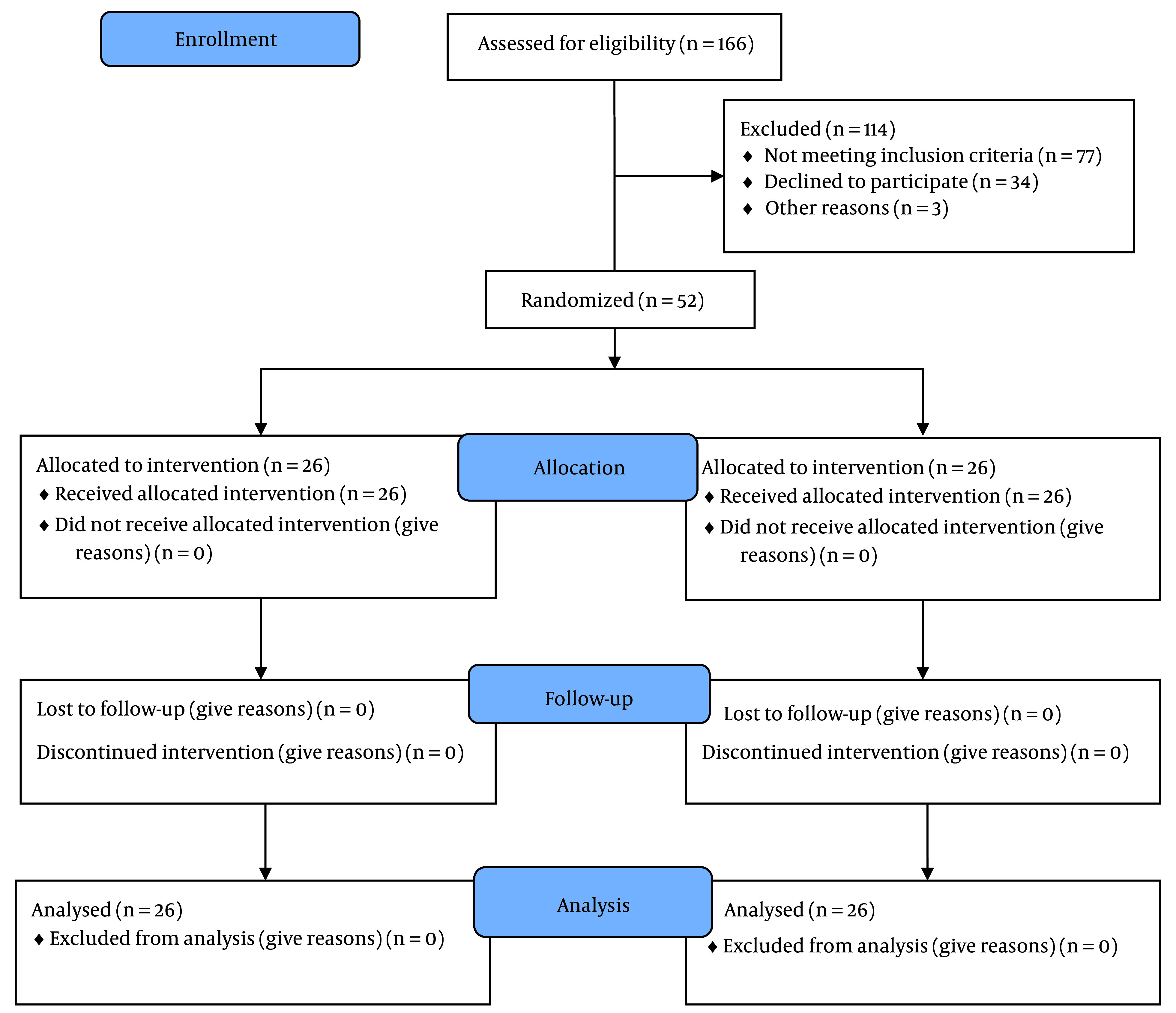
Methods: A randomized double-blinded clinical trial was conducted involving 52 PLSS patients who were randomly assigned to either the CESI group or the S1-TFESI group. The patients were positioned prone. A linear transducer with a curve at a low frequency (2 - 5 MHz) was used to visualize the area. An aseptically prepared puncture site was used to insert a 2- to 5-MHz curved ultrasound probe with an ultrasound gel to identify the articular processes of the lower lumbar vertebrae and the posterior sacral surface. The probe was then positioned longitudinally to the para-sacral area, about 2 cm lateral to the midline. The articular process represented the L5/S1 level at the farthest caudal side, and the S1 posterior sacral foramen was represented by the concavity at the posterior sacral surface that was somewhat caudal. The probe was angled caudally to provide enough room for the needle to enter the S1 foramen. The injection site for the needle tip was the S1 foramen. A combination of triamcinolone (40 mg, 1 mL), normal saline (2 mL), and ropivacaine (0.2%) was administered. For TFS1 ESI, 5 mL of the combination was used. For CESI, the sacral hiatus was palpated in the prone position, and a linear high-frequency transducer was placed transversely to obtain a transverse view of the sacral hiatus. A combination of triamcinolone 40 mg and ropivacaine (0.2%) totaling 10 mL was employed. The Numerical Rating Scale (NRS) and Oswestry Disability Index (ODI) were used to assess patients' preoperative and postoperative conditions, and adverse events were recorded. Follow-up was conducted one week and one month after the procedures.
Results: In both groups, NRS and ODI scores decreased at different time points after treatment, compared to baseline (P < 0.001). The CESI group had lower median ODI scores after one week and one month, although this difference did not reach statistical significance (P = 0.334). Despite similar baseline NRS ratings, the CESI group had statistically significantly lower mean NRS scores at one week and one month (P < 0.001).
Conclusions: The current study demonstrated that both CESI and TFESI treatments for PLSS following lumbar discectomy are effective and safe. These procedures can alleviate pain and reduce disability. Although the success rates of the two procedures are comparable, CESI appears to be more successful in reducing pain at the one-week and one-month follow-up.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


