Coronary revascularization and sex differences in cardiovascular mortality after myocardial infarction in 12 high and middle-income European countries.
Edina Cenko, Jinsung Yoon, Maria Bergami, Chris P Gale, Zorana Vasiljevic, Marija Vavlukis, Sasko Kedev, Davor Miličić, Maria Dorobantu, Lina Badimon, Olivia Manfrini, Raffaele Bugiardini
{"title":"Coronary revascularization and sex differences in cardiovascular mortality after myocardial infarction in 12 high and middle-income European countries.","authors":"Edina Cenko, Jinsung Yoon, Maria Bergami, Chris P Gale, Zorana Vasiljevic, Marija Vavlukis, Sasko Kedev, Davor Miličić, Maria Dorobantu, Lina Badimon, Olivia Manfrini, Raffaele Bugiardini","doi":"10.1093/ehjqcco/qcae035","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Existing data on female sex and excess cardiovascular mortality after myocardial infarction (MI) mostly come from high-income countries (HICs). This study aimed to investigate how sex disparities in treatments and outcomes vary across countries with different income levels.</p><p><strong>Methods: </strong>Data from the ISACS Archives registry included 22 087 MI patients from 6 HICs and 6 middle-income countries (MICs). MI data were disaggregated by clinical presentation: ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation myocardial infarction (NSTEMI). The primary outcome was 30-day mortality.</p><p><strong>Results: </strong>Among STEMI patients, women in MICs had nearly double the 30-day mortality rate of men [12.4% vs. 5.8%; adjusted risk ratio (RR) 2.30, 95% CI 1.98-2.68]. This difference was less pronounced in HICs (6.8% vs. 5.1%; RR 1.36, 95% CI 1.05-1.75). Despite more frequent treatments and timely revascularization in MICs, sex-based mortality differences persisted even after revascularization (8.0% vs. 4.1%; RR 2.05, 95% CI, 1.68-2.50 in MICs and 5.6% vs. 2.6%; RR 2.17, 95% CI, 1.48-3.18) in HICs. Additionally, women from MICs had higher diabetes rates compared to HICs (31.8% vs. 25.1%, standardized difference = 0.15). NSTEMI outcomes were relatively similar between sexes and income groups.</p><p><strong>Conclusions: </strong>Sex disparities in mortality rates following STEMI are more pronounced in MICs compared to HICs. These disparities cannot be solely attributed to sex-related inequities in revascularization. Variations in mortality may also be influenced by sex differences in socioeconomic factors and baseline comorbidities.</p>","PeriodicalId":11869,"journal":{"name":"European Heart Journal - Quality of Care and Clinical Outcomes","volume":" ","pages":"719-729"},"PeriodicalIF":4.6000,"publicationDate":"2025-09-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12445642/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal - Quality of Care and Clinical Outcomes","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ehjqcco/qcae035","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Existing data on female sex and excess cardiovascular mortality after myocardial infarction (MI) mostly come from high-income countries (HICs). This study aimed to investigate how sex disparities in treatments and outcomes vary across countries with different income levels.
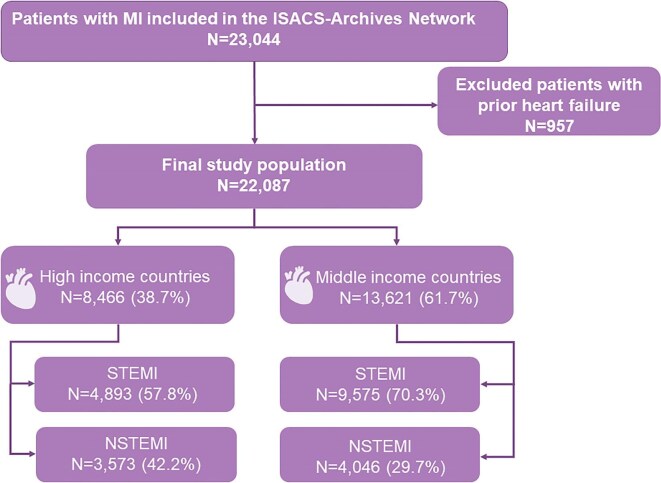
Methods: Data from the ISACS Archives registry included 22 087 MI patients from 6 HICs and 6 middle-income countries (MICs). MI data were disaggregated by clinical presentation: ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation myocardial infarction (NSTEMI). The primary outcome was 30-day mortality.
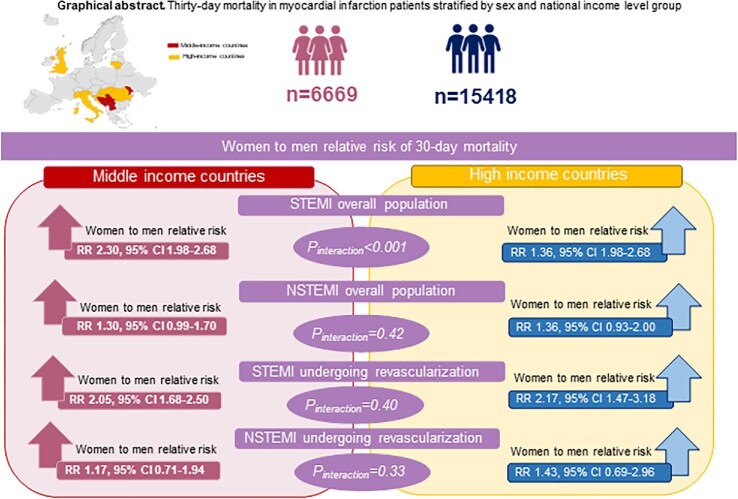
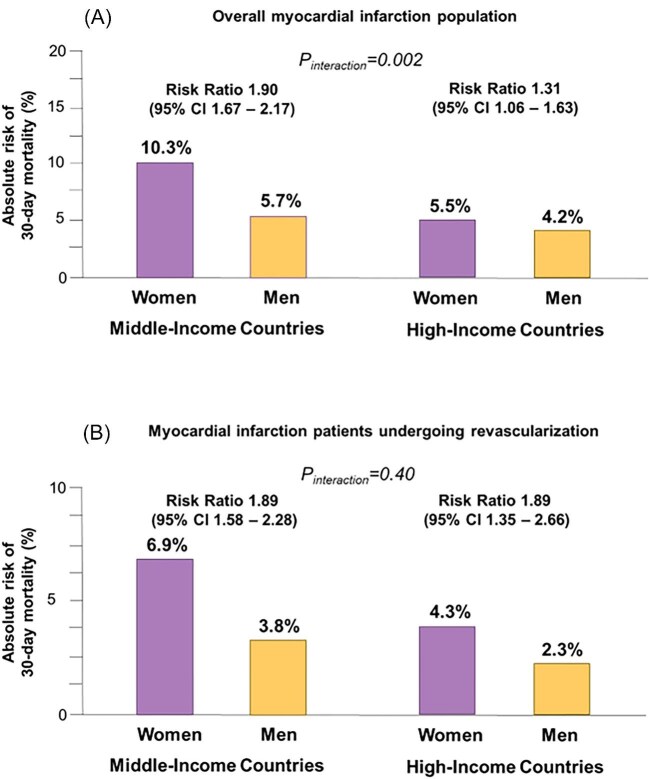
Results: Among STEMI patients, women in MICs had nearly double the 30-day mortality rate of men [12.4% vs. 5.8%; adjusted risk ratio (RR) 2.30, 95% CI 1.98-2.68]. This difference was less pronounced in HICs (6.8% vs. 5.1%; RR 1.36, 95% CI 1.05-1.75). Despite more frequent treatments and timely revascularization in MICs, sex-based mortality differences persisted even after revascularization (8.0% vs. 4.1%; RR 2.05, 95% CI, 1.68-2.50 in MICs and 5.6% vs. 2.6%; RR 2.17, 95% CI, 1.48-3.18) in HICs. Additionally, women from MICs had higher diabetes rates compared to HICs (31.8% vs. 25.1%, standardized difference = 0.15). NSTEMI outcomes were relatively similar between sexes and income groups.
Conclusions: Sex disparities in mortality rates following STEMI are more pronounced in MICs compared to HICs. These disparities cannot be solely attributed to sex-related inequities in revascularization. Variations in mortality may also be influenced by sex differences in socioeconomic factors and baseline comorbidities.
期刊介绍:
European Heart Journal - Quality of Care & Clinical Outcomes is an English language, peer-reviewed journal dedicated to publishing cardiovascular outcomes research. It serves as an official journal of the European Society of Cardiology and maintains a close alliance with the European Heart Health Institute. The journal disseminates original research and topical reviews contributed by health scientists globally, with a focus on the quality of care and its impact on cardiovascular outcomes at the hospital, national, and international levels. It provides a platform for presenting the most outstanding cardiovascular outcomes research to influence cardiovascular public health policy on a global scale. Additionally, the journal aims to motivate young investigators and foster the growth of the outcomes research community.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


