Caitlyn F. Connor, Alisia A. W. Weyna, Nicole L. Gottdenker, Erin L. Beasley, Samantha N. Schlemmer
{"title":"What is your diagnosis? Urine from a horse","authors":"Caitlyn F. Connor, Alisia A. W. Weyna, Nicole L. Gottdenker, Erin L. Beasley, Samantha N. Schlemmer","doi":"10.1111/vcp.13346","DOIUrl":null,"url":null,"abstract":"<p>A 9-year-old Arabian gelding was referred for a 4-day history of hyporexia and pigmenturia after a 2-hour trail ride with severe azotemia (creatinine 9.6 mg/dL, RI: 1.0–2.0; BUN 65 mg/dL, RI: 8–26) and increased muscle enzyme activities (AST 10 167 IU/L, RI: 148–420; Creatine kinase [CK] 22 266 IU/L, RI: 45–360) noted on day 2. Prior treatment included flunixin meglumine.</p><p>The horse appeared painful with diffuse muscle fasciculations, with no other exam abnormalities. A CBC revealed a mild leukocytosis (mild mature neutrophilia); the erythron and thrombon were unremarkable. Serum biochemistry demonstrated persistent azotemia (creatinine 13.5 mg/dL, RI: 0.8–1.5), increased CK (8471 U/L, RI: 186–760), high anion gap (27, RI: 10–19), hyponatremia (128 mmol/L, RI: 132–140), hypochloremia (80 mmol/L, RI: 95–103), hyperkalemia (5.2 mmol/L, RI: 2.6–4.7), hyperalbuminemia (3.4 g/dL, RI: 2.5–3.3), hyperglycemia (125 mg/dL, RI: 70–113) and hypercalcemia (14.4 mg/dL, RI: 11–13.4); free/ionized calcium was 1.53 mmol/L (RI: 1.09–1.67).</p><p>Cystoscopy revealed red filamentous material pooling in the urine (Figure 1A,B). The urine was isosthenuric (USG 1.010) and alkaline (pH 8.0) with 1+ protein and large blood. Unstained sediment contained 10–50 RBC/hpf, 10–20 WBC/hpf, many transitional epithelial cells, 0–5/lpf linear structures (Figure 1C), rare calcium carbonate crystals, and moderate mucus threads.</p><p>The minimum database findings were suggestive of inflammation/stress, dehydration, muscle injury, and renal injury/insufficiency. The presence of macroscopic urinary casts was striking and unique. In general, urinary casts are rare in herbivores due to alkalinuria.<span><sup>1</sup></span> Cellular and granular casts are abnormal and indicate acute renal tubular injury. Cellular casts are defined by their cell composition: epithelial casts indicate renal tubular degeneration or necrosis secondary to severe dehydration, ischemia/infarction, nephrotoxicity, or pigment nephropathy; leukocyte casts imply tubulointerstitial inflammation (eg, pyelonephritis); and erythrocyte casts indicate intrarenal hemorrhage.<span><sup>1-3</sup></span> Granular casts form from the degeneration of cellular casts. In this case, the granular-appearing casts were presumed to represent breakdown products/proteins from erythrocytes (hemoglobin) and muscle (myoglobin). Hemoglobin casts occur with intravascular hemolysis and renal hemorrhage, whereas myoglobin casts indicate severe muscle injury or necrosis.<span><sup>2, 3</sup></span> These proteins can have a similar appearance on routine stains and can be delineated with Okajima stain (hemoglobin stains orange to orange-red) and myoglobin IHC (specific to myoglobin).</p><p>Endogenous injury from myoglobin or hemoglobin (pigment nephropathy) can result in renal tubular injury due to altered blood flow, cast formation, tubular obstruction, and oxidative injury.<span><sup>1-3</sup></span> Given the history of a trail ride preceding the hyporexia and pigmenturia, moderately increased muscle enzyme activities, and positive immunoreactivity to myoglobin IHC, the horse likely developed pigment nephropathy from myoglobinuria, with secondary intraluminal erythrocytes and hemoglobin from renal hemorrhage and tubular necrosis. CK activity >1000 IU/L or 3–5 times the upper reference limit is often indicative of acute muscle necrosis.<span><sup>4, 5</sup></span> Additionally, peak CK activity will occur 4–6 h after muscle injury.<span><sup>5</sup></span> Therefore, the historical increase in muscle enzyme activity reported by the referring veterinarian 2 days after the onset of clinical signs suggests that the peak CK activity was likely much greater, supporting acute muscle ischemia/necrosis and subsequent myoglobinuria and myoglobin cast formation. Furthermore, this horse did not develop anemia throughout the entire clinical course, so causes of primary hemoglobinuric nephropathy (eg, immune-mediated hemolytic anemia, red maple leaf, or <i>Allium</i> species ingestion)<span><sup>1-3</sup></span> were considered unlikely. Although only two doses of flunixin were given 24 h apart, the nephrotoxic potential would be greater if the horse had concurrent dehydration/hypovolemia and/or renal injury/insufficiency,<span><sup>1, 2</sup></span> which may have contributed to the renal injury in this case.</p><p>Myoglobinuria may stem from exertional myopathies (eg, sporadic or recurrent exertional rhabdomyolysis, myofibrillar myopathy, polysaccharide storage myopathy), trauma, immune-mediated myopathies, malignant hyperthermia, clostridial myonecrosis, selenium deficiency, toxin (ionophore) ingestions, atypical myopathy/myoglobinuria, or even heat exhaustion.<span><sup>3-5</sup></span> In this case, it is unknown if there was any prior history of tying-up episodes that may support an underlying primary myopathy. Arabians are included in the performance horses (along with Thoroughbreds and standardbreds) that can develop rhabdomyolysis without underlying myopathy.<span><sup>4, 5</sup></span> Given the lack of gross muscle abnormalities in this case, these tissues were not collected at the time of necropsy, precluding a more definitive cause of myopathy.</p><p>In all, this case highlights the unique gross and microscopic morphology of pigment-containing casts in a horse with acute kidney injury presumed secondary to myopathy. These casts should not be overlooked as contaminants and should be included in the microscopic review, as they indicate renal pathology, and special stains can be used to differentiate hemoglobin and myoglobin pigments.</p><p>The authors have indicated that they have no affiliations or financial involvement with any organization or entity with a financial interest in, or in financial competition with, the subject matter or materials discussed in this article.</p>","PeriodicalId":23593,"journal":{"name":"Veterinary clinical pathology","volume":"53 S2","pages":"142-145"},"PeriodicalIF":1.1000,"publicationDate":"2024-04-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/vcp.13346","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Veterinary clinical pathology","FirstCategoryId":"97","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/vcp.13346","RegionNum":4,"RegionCategory":"农林科学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"VETERINARY SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
A 9-year-old Arabian gelding was referred for a 4-day history of hyporexia and pigmenturia after a 2-hour trail ride with severe azotemia (creatinine 9.6 mg/dL, RI: 1.0–2.0; BUN 65 mg/dL, RI: 8–26) and increased muscle enzyme activities (AST 10 167 IU/L, RI: 148–420; Creatine kinase [CK] 22 266 IU/L, RI: 45–360) noted on day 2. Prior treatment included flunixin meglumine.
The horse appeared painful with diffuse muscle fasciculations, with no other exam abnormalities. A CBC revealed a mild leukocytosis (mild mature neutrophilia); the erythron and thrombon were unremarkable. Serum biochemistry demonstrated persistent azotemia (creatinine 13.5 mg/dL, RI: 0.8–1.5), increased CK (8471 U/L, RI: 186–760), high anion gap (27, RI: 10–19), hyponatremia (128 mmol/L, RI: 132–140), hypochloremia (80 mmol/L, RI: 95–103), hyperkalemia (5.2 mmol/L, RI: 2.6–4.7), hyperalbuminemia (3.4 g/dL, RI: 2.5–3.3), hyperglycemia (125 mg/dL, RI: 70–113) and hypercalcemia (14.4 mg/dL, RI: 11–13.4); free/ionized calcium was 1.53 mmol/L (RI: 1.09–1.67).
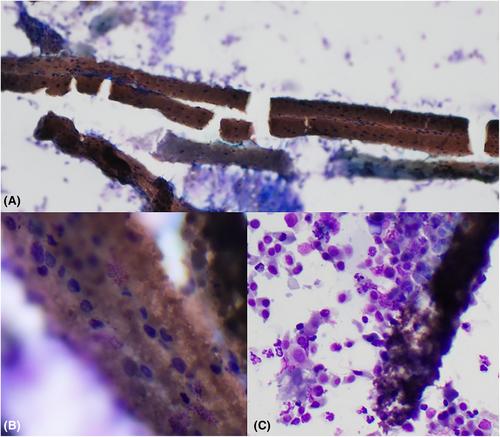
Cystoscopy revealed red filamentous material pooling in the urine (Figure 1A,B). The urine was isosthenuric (USG 1.010) and alkaline (pH 8.0) with 1+ protein and large blood. Unstained sediment contained 10–50 RBC/hpf, 10–20 WBC/hpf, many transitional epithelial cells, 0–5/lpf linear structures (Figure 1C), rare calcium carbonate crystals, and moderate mucus threads.
The minimum database findings were suggestive of inflammation/stress, dehydration, muscle injury, and renal injury/insufficiency. The presence of macroscopic urinary casts was striking and unique. In general, urinary casts are rare in herbivores due to alkalinuria.1 Cellular and granular casts are abnormal and indicate acute renal tubular injury. Cellular casts are defined by their cell composition: epithelial casts indicate renal tubular degeneration or necrosis secondary to severe dehydration, ischemia/infarction, nephrotoxicity, or pigment nephropathy; leukocyte casts imply tubulointerstitial inflammation (eg, pyelonephritis); and erythrocyte casts indicate intrarenal hemorrhage.1-3 Granular casts form from the degeneration of cellular casts. In this case, the granular-appearing casts were presumed to represent breakdown products/proteins from erythrocytes (hemoglobin) and muscle (myoglobin). Hemoglobin casts occur with intravascular hemolysis and renal hemorrhage, whereas myoglobin casts indicate severe muscle injury or necrosis.2, 3 These proteins can have a similar appearance on routine stains and can be delineated with Okajima stain (hemoglobin stains orange to orange-red) and myoglobin IHC (specific to myoglobin).
Endogenous injury from myoglobin or hemoglobin (pigment nephropathy) can result in renal tubular injury due to altered blood flow, cast formation, tubular obstruction, and oxidative injury.1-3 Given the history of a trail ride preceding the hyporexia and pigmenturia, moderately increased muscle enzyme activities, and positive immunoreactivity to myoglobin IHC, the horse likely developed pigment nephropathy from myoglobinuria, with secondary intraluminal erythrocytes and hemoglobin from renal hemorrhage and tubular necrosis. CK activity >1000 IU/L or 3–5 times the upper reference limit is often indicative of acute muscle necrosis.4, 5 Additionally, peak CK activity will occur 4–6 h after muscle injury.5 Therefore, the historical increase in muscle enzyme activity reported by the referring veterinarian 2 days after the onset of clinical signs suggests that the peak CK activity was likely much greater, supporting acute muscle ischemia/necrosis and subsequent myoglobinuria and myoglobin cast formation. Furthermore, this horse did not develop anemia throughout the entire clinical course, so causes of primary hemoglobinuric nephropathy (eg, immune-mediated hemolytic anemia, red maple leaf, or Allium species ingestion)1-3 were considered unlikely. Although only two doses of flunixin were given 24 h apart, the nephrotoxic potential would be greater if the horse had concurrent dehydration/hypovolemia and/or renal injury/insufficiency,1, 2 which may have contributed to the renal injury in this case.
Myoglobinuria may stem from exertional myopathies (eg, sporadic or recurrent exertional rhabdomyolysis, myofibrillar myopathy, polysaccharide storage myopathy), trauma, immune-mediated myopathies, malignant hyperthermia, clostridial myonecrosis, selenium deficiency, toxin (ionophore) ingestions, atypical myopathy/myoglobinuria, or even heat exhaustion.3-5 In this case, it is unknown if there was any prior history of tying-up episodes that may support an underlying primary myopathy. Arabians are included in the performance horses (along with Thoroughbreds and standardbreds) that can develop rhabdomyolysis without underlying myopathy.4, 5 Given the lack of gross muscle abnormalities in this case, these tissues were not collected at the time of necropsy, precluding a more definitive cause of myopathy.
In all, this case highlights the unique gross and microscopic morphology of pigment-containing casts in a horse with acute kidney injury presumed secondary to myopathy. These casts should not be overlooked as contaminants and should be included in the microscopic review, as they indicate renal pathology, and special stains can be used to differentiate hemoglobin and myoglobin pigments.
The authors have indicated that they have no affiliations or financial involvement with any organization or entity with a financial interest in, or in financial competition with, the subject matter or materials discussed in this article.
期刊介绍:
Veterinary Clinical Pathology is the official journal of the American Society for Veterinary Clinical Pathology (ASVCP) and the European Society of Veterinary Clinical Pathology (ESVCP). The journal''s mission is to provide an international forum for communication and discussion of scientific investigations and new developments that advance the art and science of laboratory diagnosis in animals. Veterinary Clinical Pathology welcomes original experimental research and clinical contributions involving domestic, laboratory, avian, and wildlife species in the areas of hematology, hemostasis, immunopathology, clinical chemistry, cytopathology, surgical pathology, toxicology, endocrinology, laboratory and analytical techniques, instrumentation, quality assurance, and clinical pathology education.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


