{"title":"A generalized rash in an 8-year-old patient","authors":"Ashley S. Kim, Astrid H. Lossius","doi":"10.1002/jvc2.422","DOIUrl":null,"url":null,"abstract":"<p>An 8-year-old patient was referred for a second opinion to our dermatology department from another dermatologist. The referral reported a 14-month history of therapy-resistant rash, originally treated as nummular atopic dermatitis. The patient reported spontaneous debut of an itchy rash to the extremities and trunk, with worsening of symptoms despite use of topical steroids and UVB light therapy. The rash spread gradually to the entire body, including face and scalp. Upon examination, there was a polymorphic presentation with well-demarcated red macules, small subcorneal pustules along borders, patchy hyperkeratosis and postinflammatory hyperpigmentation (Figure 1a,b). The patient also had patchy hair thinning with a ‘black dot pattern’ (Figure 2). This finding resulted in diagnostic workup to exclude fungal infection, subacute cutaneous lupus, psoriasis and secondary syphilis, in order of decreasing clinical likelihood. Skin and hair samples were both positive for dermatophyte DNA, <i>Trichophyton</i> species. Histology also reported fungal elements in the keratin layer. Treatment initiated with terbinafine 125 mg daily for 6 weeks, in addition to ketoconazole shampoo. Upon control, the patient presented with postinflammatory hyperpigmentation, however, her other symptoms had abated and she had experienced hair regrowth. Control skin samples were negative for dermatophyte DNA.</p><p>Ashley S. Kim wrote the manuscript and Astrid H. Lossius provided revisions. Both authors were involved in the workup and final diagnosis of this patient. Ashley S. Kim is the corresponding author.</p><p>The authors declare no conflict of interest.</p><p>The parents of minor patients have been given written informed consent for their child's participation in this article, as well as for the use of their child's deidentified, anonymized case details (including photographs) for publication. Ethical approval: Not applicable.</p>","PeriodicalId":94325,"journal":{"name":"JEADV clinical practice","volume":"3 4","pages":"1316-1317"},"PeriodicalIF":0.0000,"publicationDate":"2024-04-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jvc2.422","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JEADV clinical practice","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jvc2.422","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
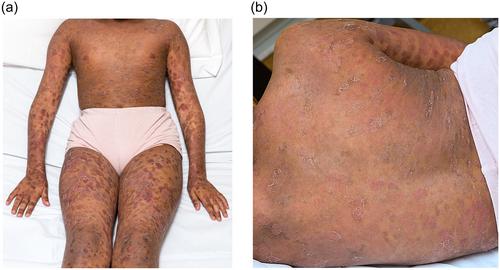
An 8-year-old patient was referred for a second opinion to our dermatology department from another dermatologist. The referral reported a 14-month history of therapy-resistant rash, originally treated as nummular atopic dermatitis. The patient reported spontaneous debut of an itchy rash to the extremities and trunk, with worsening of symptoms despite use of topical steroids and UVB light therapy. The rash spread gradually to the entire body, including face and scalp. Upon examination, there was a polymorphic presentation with well-demarcated red macules, small subcorneal pustules along borders, patchy hyperkeratosis and postinflammatory hyperpigmentation (Figure 1a,b). The patient also had patchy hair thinning with a ‘black dot pattern’ (Figure 2). This finding resulted in diagnostic workup to exclude fungal infection, subacute cutaneous lupus, psoriasis and secondary syphilis, in order of decreasing clinical likelihood. Skin and hair samples were both positive for dermatophyte DNA, Trichophyton species. Histology also reported fungal elements in the keratin layer. Treatment initiated with terbinafine 125 mg daily for 6 weeks, in addition to ketoconazole shampoo. Upon control, the patient presented with postinflammatory hyperpigmentation, however, her other symptoms had abated and she had experienced hair regrowth. Control skin samples were negative for dermatophyte DNA.
Ashley S. Kim wrote the manuscript and Astrid H. Lossius provided revisions. Both authors were involved in the workup and final diagnosis of this patient. Ashley S. Kim is the corresponding author.
The authors declare no conflict of interest.
The parents of minor patients have been given written informed consent for their child's participation in this article, as well as for the use of their child's deidentified, anonymized case details (including photographs) for publication. Ethical approval: Not applicable.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


