A follow-up study on respiratory outcomes, quality of life and performance perception of SARS-CoV-2 primary and reinfection in elite athletes: A 9-month prospective study
{"title":"A follow-up study on respiratory outcomes, quality of life and performance perception of SARS-CoV-2 primary and reinfection in elite athletes: A 9-month prospective study","authors":"Emre Karaduman, Özgür Bostancı, Sait Bilgiç","doi":"10.1002/ejsc.12109","DOIUrl":null,"url":null,"abstract":"<p>The prolonged consequences of SARS-CoV-2 on young elite athletes recovering from primary and reinfection are unclear. This study aimed to assess inspiratory/expiratory muscle strength and respiratory function at the time of spontaneous recovery at 3, 6, and 9 months after SARS-CoV-2 primary and reinfection in elite athletes. The study enrolled 25 elite male judoists, including 11 primary infection cases, five reinfection cases, and nine controls from the Türkiye Olympic Preparation Center. Inspiratory/expiratory muscle strength and respiratory function were measured, including maximal inspiratory pressure (MIP), maximal expiratory pressure (MEP), forced expiratory volume in 1 s (FEV<sub>1</sub>), forced vital capacity (FVC), FEV<sub>1</sub>/FVC, and peak expiratory flow (PEF) before and up to 9 months after SARS-CoV-2 infection in the early pre-competition preparation phases. The most common symptoms reported by reinfection cases were fatigue (80%), dyspnea (60%), and muscle/joint pain (60%), while primary infection cases reported fatigue (73%), muscle/joint pain (45%), and headache (45%). MIP decreased by −14% and MEP decreased by −13% following the SARS-CoV-2 infection in reinfection cases. Likewise, FEV<sub>1</sub> and FVC decreased by −5% and −8%, respectively; consequently, FEV<sub>1</sub>/FVC increased by 3%. Inspiratory/expiratory muscle strength and respiratory function improved rapidly after 9 months of SARS-CoV-2 infection in primary cases, whereas dysfunction persisted in reinfection cases. PEF was unaffected throughout the 9-month follow-up period. Reinfection may lead to further alterations in respiratory system relative to the primary infection, with a suspected restrictive pattern that remains dysfunctional in the third month; however, it improves significantly during a 9-month follow-up period.</p>","PeriodicalId":93999,"journal":{"name":"European journal of sport science","volume":"24 7","pages":"964-974"},"PeriodicalIF":3.0000,"publicationDate":"2024-04-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ejsc.12109","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of sport science","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ejsc.12109","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
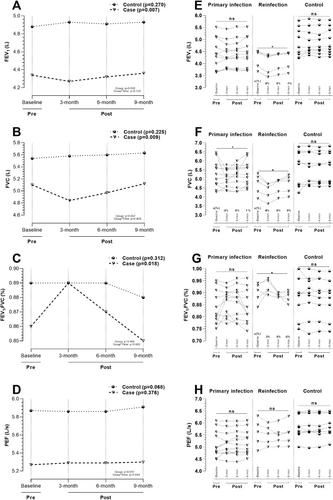
The prolonged consequences of SARS-CoV-2 on young elite athletes recovering from primary and reinfection are unclear. This study aimed to assess inspiratory/expiratory muscle strength and respiratory function at the time of spontaneous recovery at 3, 6, and 9 months after SARS-CoV-2 primary and reinfection in elite athletes. The study enrolled 25 elite male judoists, including 11 primary infection cases, five reinfection cases, and nine controls from the Türkiye Olympic Preparation Center. Inspiratory/expiratory muscle strength and respiratory function were measured, including maximal inspiratory pressure (MIP), maximal expiratory pressure (MEP), forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), FEV1/FVC, and peak expiratory flow (PEF) before and up to 9 months after SARS-CoV-2 infection in the early pre-competition preparation phases. The most common symptoms reported by reinfection cases were fatigue (80%), dyspnea (60%), and muscle/joint pain (60%), while primary infection cases reported fatigue (73%), muscle/joint pain (45%), and headache (45%). MIP decreased by −14% and MEP decreased by −13% following the SARS-CoV-2 infection in reinfection cases. Likewise, FEV1 and FVC decreased by −5% and −8%, respectively; consequently, FEV1/FVC increased by 3%. Inspiratory/expiratory muscle strength and respiratory function improved rapidly after 9 months of SARS-CoV-2 infection in primary cases, whereas dysfunction persisted in reinfection cases. PEF was unaffected throughout the 9-month follow-up period. Reinfection may lead to further alterations in respiratory system relative to the primary infection, with a suspected restrictive pattern that remains dysfunctional in the third month; however, it improves significantly during a 9-month follow-up period.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


