Chao Li PhD, Richard A. Preston MD, Emily Dumas PhD, Andrew Beelen MD, Thomas C. Marbury MD
{"title":"Effect of Hepatic Impairment on Trilaciclib Pharmacokinetics","authors":"Chao Li PhD, Richard A. Preston MD, Emily Dumas PhD, Andrew Beelen MD, Thomas C. Marbury MD","doi":"10.1002/jcph.2435","DOIUrl":null,"url":null,"abstract":"<p>Trilaciclib is a first-in-class, intravenous cyclin-dependent kinase 4 and 6 inhibitor approved for reducing the incidence of chemotherapy-induced myelosuppression in adult patients with extensive-stage small cell lung cancer receiving a platinum/etoposide-containing or topotecan-containing regimen. No dose adjustment is recommended for participants with mild hepatic impairment (HI) based on previous population pharmacokinetic (PK) analysis. This open-label, parallel-group study examined the impact of moderate and severe HI on the PK of trilaciclib. The study employed a reduced study design. Participants with moderate (Child–Pugh B, n = 8) and severe (Child–Pugh C, n = 5) HI and matched healthy controls (n = 11) received a single intravenous dose of trilaciclib 100 mg/m<sup>2</sup>. The unbound fraction of trilaciclib was comparable between the HI groups and the matched healthy control group. The unbound trilaciclib extent of exposure (i.e., area under the concentration-time curve) in participants with moderate and severe HI was ∼40% and ∼60% higher, respectively, compared with healthy matched controls based on Child–Pugh classification. Ad hoc analysis using National Cancer Institute classification showed similar results. The US Food and Drug Administration-approved trilaciclib dose of 240 mg/m<sup>2</sup> should be reduced by ∼30%, to 170 mg/m<sup>2</sup>, for patients with moderate or severe HI.</p>","PeriodicalId":22751,"journal":{"name":"The Journal of Clinical Pharmacology","volume":"64 8","pages":"975-983"},"PeriodicalIF":0.0000,"publicationDate":"2024-04-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jcph.2435","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Journal of Clinical Pharmacology","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jcph.2435","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
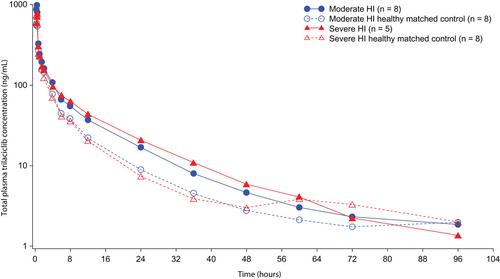
Trilaciclib is a first-in-class, intravenous cyclin-dependent kinase 4 and 6 inhibitor approved for reducing the incidence of chemotherapy-induced myelosuppression in adult patients with extensive-stage small cell lung cancer receiving a platinum/etoposide-containing or topotecan-containing regimen. No dose adjustment is recommended for participants with mild hepatic impairment (HI) based on previous population pharmacokinetic (PK) analysis. This open-label, parallel-group study examined the impact of moderate and severe HI on the PK of trilaciclib. The study employed a reduced study design. Participants with moderate (Child–Pugh B, n = 8) and severe (Child–Pugh C, n = 5) HI and matched healthy controls (n = 11) received a single intravenous dose of trilaciclib 100 mg/m2. The unbound fraction of trilaciclib was comparable between the HI groups and the matched healthy control group. The unbound trilaciclib extent of exposure (i.e., area under the concentration-time curve) in participants with moderate and severe HI was ∼40% and ∼60% higher, respectively, compared with healthy matched controls based on Child–Pugh classification. Ad hoc analysis using National Cancer Institute classification showed similar results. The US Food and Drug Administration-approved trilaciclib dose of 240 mg/m2 should be reduced by ∼30%, to 170 mg/m2, for patients with moderate or severe HI.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


