Interaction of left ventricular size with the outcome of cardiac resynchronization therapy in Japanese patients
Abstract
Background
We analyzed the influence of the QRS duration (QRSd) to LV end-diastolic volume (LVEDV) ratio on cardiac resynchronization therapy (CRT) outcomes in heart failure patients classified as III/IV per the New York Heart Association (NYHA) and with small body size.
Hypothesis
We proposed the hypothesis that the QRSd/LV size ratio is a better index of the CRT substrate.
Methods
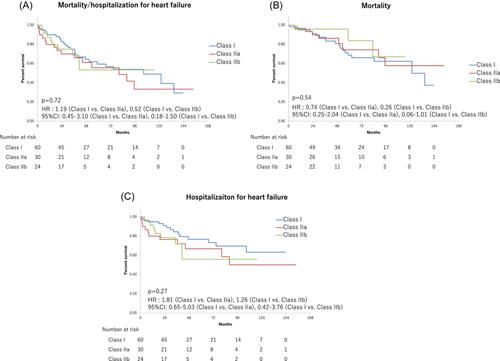
We enrolled 114 patients with advanced heart failure (NYHA class III/IV, and LV ejection fraction >35%) who received a CRT device, including those with left bundle branch block (LBBB) and QRSd ≥120 milliseconds (n = 60), non-LBBB and QRSd ≥150 milliseconds (n = 30) and non-LBBB and QRSd of 120−149 milliseconds (n = 24).
Results
Over a mean follow-up period of 65 ± 58 months, the incidence of the primary endpoint, a composite of all-cause death and hospitalization for heart failure, showed no significant intergroup difference (43.3% vs. 50.0% vs. 37.5%, respectively, p = .72). Similarly, among 104 patients with QRSd/LVEDV ≥ 0.67 (n = 54) and QRSd/LVEDV < 0.67 (n = 52), no significant differences were observed in the incidence of the primary endpoint (35.1% vs. 51.9%, p = .49). Nevertheless, patients with QRSd/LVEDV ≥ 0.67 showed better survival than those with QRSd/LVEDV < 0.67 (14.8% vs. 34.6%, p = .0024).
Conclusion
Advanced HF patients with a higher QRSd/LVEDV ratio showed better survival in this small-body–size population. Thus, the risk is concentrated among those with a larger QRSd, and patients with a relatively smaller left ventricular size appeared to benefit from CRT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


