{"title":"Predictive role of hepatic venous pressure gradient in bleeding events among patients with cirrhosis undergoing orthotopic liver transplantation","authors":"Mikhael Giabicani , Pauline Joly , Stéphanie Sigaut , Clara Timsit , Pauline Devauchelle , Fédérica Dondero , François Durand , Pierre Antoine Froissant , Myriam Lamamri , Audrey Payancé , Aymeric Restoux , Olivier Roux , Tristan Thibault-Sogorb , Shantha Ram Valainathan , Mickaël Lesurtel , Pierre-Emmanuel Rautou , Emmanuel Weiss","doi":"10.1016/j.jhepr.2024.101051","DOIUrl":null,"url":null,"abstract":"<div><h3>Background & Aims</h3><p>Major bleeding events during orthotopic liver transplantation (OLT) are associated with poor outcomes. The proportion of this risk related to portal hypertension is unclear. Hepatic venous pressure gradient (HVPG) is the gold standard for estimating portal hypertension. The aim of this study was to analyze the ability of HVPG to predict intraoperative major bleeding events during OLT in patients with cirrhosis.</p></div><div><h3>Methods</h3><p>We retrospectively analyzed a prospective database including all patients with cirrhosis who underwent OLT between 2010 and 2020 and had liver and right heart catheterizations as part of their pre-transplant assessment. The primary endpoint was the occurrence of an intraoperative major bleeding event.</p></div><div><h3>Results</h3><p>The 468 included patients had a median HVPG of 17 mmHg [interquartile range, 13-22] and a median MELD on the day of OLT of 16 [11-24]. Intraoperative red blood cell transfusion was required in 72% of the patients (median 2 units transfused), with a median blood loss of 1,000 ml [575-1,500]. Major intraoperative bleeding occurred in 156 patients (33%) and was associated with HVPG, preoperative hemoglobin level, severity of cirrhosis at the time of OLT (MELD score, ascites, encephalopathy), hemostasis impairment (thrombocytopenia, lower fibrinogen levels), and complications of cirrhosis (sepsis, acute-on-chronic liver failure). By multivariable regression analysis with backward elimination, HVPG, preoperative hemoglobin level, MELD score, and tranexamic acid infusion were associated with the primary endpoint. Three categories of patients were identified according to HVPG: low-risk (HVPG <16 mmHg), high-risk (HVGP ≥16 mmHg), and very high-risk (HVPG ≥20 mmHg).</p></div><div><h3>Conclusions</h3><p>HVPG predicted major bleeding events in patients with cirrhosis undergoing OLT. Including HVPG as part of pre-transplant assessment might enable better anticipation of the intraoperative course.</p></div><div><h3>Impact and implications</h3><p>Major bleeding events during orthotopic liver transplantation (OLT) are associated with poor outcomes but the proportion of this risk related to portal hypertension is unclear. Our work shows that hepatic venous pressure gradient (HVPG), the gold standard for estimating portal hypertension, is a strong predictor of major bleeding events and blood loss volume in patients with cirrhosis undergoing OLT. Three groups of patients can be identified according to their risk of major bleeding events: low-risk patients with HVPG <16 mmHg, high-risk patients with HVPG ≥16 mmHg, and very high-risk patients with HVPG ≥20 mmHg. HVPG could be systematically included in the pre-transplant assessment to anticipate intraoperative course and tailor patient management.</p></div>","PeriodicalId":14764,"journal":{"name":"JHEP Reports","volume":"6 6","pages":"Article 101051"},"PeriodicalIF":9.5000,"publicationDate":"2024-02-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2589555924000521/pdfft?md5=f8e70d7bfcc17e1b76098bcbe70de7c2&pid=1-s2.0-S2589555924000521-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JHEP Reports","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2589555924000521","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background & Aims
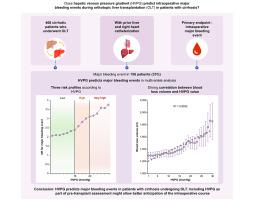
Major bleeding events during orthotopic liver transplantation (OLT) are associated with poor outcomes. The proportion of this risk related to portal hypertension is unclear. Hepatic venous pressure gradient (HVPG) is the gold standard for estimating portal hypertension. The aim of this study was to analyze the ability of HVPG to predict intraoperative major bleeding events during OLT in patients with cirrhosis.
Methods
We retrospectively analyzed a prospective database including all patients with cirrhosis who underwent OLT between 2010 and 2020 and had liver and right heart catheterizations as part of their pre-transplant assessment. The primary endpoint was the occurrence of an intraoperative major bleeding event.
Results
The 468 included patients had a median HVPG of 17 mmHg [interquartile range, 13-22] and a median MELD on the day of OLT of 16 [11-24]. Intraoperative red blood cell transfusion was required in 72% of the patients (median 2 units transfused), with a median blood loss of 1,000 ml [575-1,500]. Major intraoperative bleeding occurred in 156 patients (33%) and was associated with HVPG, preoperative hemoglobin level, severity of cirrhosis at the time of OLT (MELD score, ascites, encephalopathy), hemostasis impairment (thrombocytopenia, lower fibrinogen levels), and complications of cirrhosis (sepsis, acute-on-chronic liver failure). By multivariable regression analysis with backward elimination, HVPG, preoperative hemoglobin level, MELD score, and tranexamic acid infusion were associated with the primary endpoint. Three categories of patients were identified according to HVPG: low-risk (HVPG <16 mmHg), high-risk (HVGP ≥16 mmHg), and very high-risk (HVPG ≥20 mmHg).
Conclusions
HVPG predicted major bleeding events in patients with cirrhosis undergoing OLT. Including HVPG as part of pre-transplant assessment might enable better anticipation of the intraoperative course.
Impact and implications
Major bleeding events during orthotopic liver transplantation (OLT) are associated with poor outcomes but the proportion of this risk related to portal hypertension is unclear. Our work shows that hepatic venous pressure gradient (HVPG), the gold standard for estimating portal hypertension, is a strong predictor of major bleeding events and blood loss volume in patients with cirrhosis undergoing OLT. Three groups of patients can be identified according to their risk of major bleeding events: low-risk patients with HVPG <16 mmHg, high-risk patients with HVPG ≥16 mmHg, and very high-risk patients with HVPG ≥20 mmHg. HVPG could be systematically included in the pre-transplant assessment to anticipate intraoperative course and tailor patient management.
期刊介绍:
JHEP Reports is an open access journal that is affiliated with the European Association for the Study of the Liver (EASL). It serves as a companion journal to the highly respected Journal of Hepatology.
The primary objective of JHEP Reports is to publish original papers and reviews that contribute to the advancement of knowledge in the field of liver diseases. The journal covers a wide range of topics, including basic, translational, and clinical research. It also focuses on global issues in hepatology, with particular emphasis on areas such as clinical trials, novel diagnostics, precision medicine and therapeutics, cancer research, cellular and molecular studies, artificial intelligence, microbiome research, epidemiology, and cutting-edge technologies.
In summary, JHEP Reports is dedicated to promoting scientific discoveries and innovations in liver diseases through the publication of high-quality research papers and reviews covering various aspects of hepatology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


