T. Telecan , I. Andras , N. Crousen , E.D. Cata , P. Medan , D.V. Stanca , A. Territo , I. Coman , N. Crisan
{"title":"Laparoscopic approach for xanthogranulomatous pyelonephritis and pyonephrosis","authors":"T. Telecan , I. Andras , N. Crousen , E.D. Cata , P. Medan , D.V. Stanca , A. Territo , I. Coman , N. Crisan","doi":"10.1016/j.acuroe.2024.03.001","DOIUrl":null,"url":null,"abstract":"<div><h3>Introduction</h3><p>Xanthogranulomatous pyelonephritis (XGPN) is a rare form of chronic renal inflammation, caused by long-term obstruction of the urinary tract. Pyonephrosis is a severe suppurative complication of acute obstructive pyelonephritis. Although minimally invasive approaches have many advantages, the safe dissection of the kidney may not be always achievable.</p></div><div><h3>Materials and methods</h3><p>We reviewed 27 cases diagnosed with either XGPN or pyonephrosis, who underwent laparoscopic total nephrectomy between October 2016 and March 2022 in our department. All interventions were performed using the Karl Storz 3D laparoscopic system. The surgical approach was standard transperitoneal nephrectomy for the majority of XGPN, while pyonephrosis cases were carried out in a retroperitoneally. All procedures were performed or supervised by the same surgeon.</p></div><div><h3>Results</h3><p>The mean operative time was 269.85 minutes (range 145–360). The mean hemoglobin drop after surgery was 1.41 g/dl (range 0.3–2.3 g/dl). Difficult dissection was encountered in 13 cases (48.14%). Nine out of 13 interventions were carried out in a complete intracorporeal fashion, while conversion to open surgery was needed in 4 cases. Vascular complications involving the major blood vessels comprised of one case of inferior vena cava (IVC) tear. Digestive tract-related complications comprised two fistulas of the descending colon and one peritoneal breach. Multiorgan resection was performed in 6 cases.</p></div><div><h3>Conclusion</h3><p>Total nephrectomy in cases of XGPN and pyonephrosis is a challenging procedure. The laparoscopic approach is feasible, as most complications are resolved intracorporeally. However, it may remain reserved for large-volume centers with experienced surgeons.</p></div>","PeriodicalId":94291,"journal":{"name":"Actas urologicas espanolas","volume":"48 6","pages":"Pages 476-483"},"PeriodicalIF":0.0000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Actas urologicas espanolas","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S217357862400026X","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction
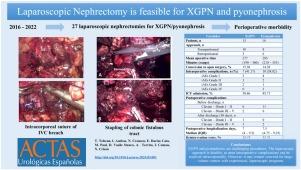
Xanthogranulomatous pyelonephritis (XGPN) is a rare form of chronic renal inflammation, caused by long-term obstruction of the urinary tract. Pyonephrosis is a severe suppurative complication of acute obstructive pyelonephritis. Although minimally invasive approaches have many advantages, the safe dissection of the kidney may not be always achievable.
Materials and methods
We reviewed 27 cases diagnosed with either XGPN or pyonephrosis, who underwent laparoscopic total nephrectomy between October 2016 and March 2022 in our department. All interventions were performed using the Karl Storz 3D laparoscopic system. The surgical approach was standard transperitoneal nephrectomy for the majority of XGPN, while pyonephrosis cases were carried out in a retroperitoneally. All procedures were performed or supervised by the same surgeon.
Results
The mean operative time was 269.85 minutes (range 145–360). The mean hemoglobin drop after surgery was 1.41 g/dl (range 0.3–2.3 g/dl). Difficult dissection was encountered in 13 cases (48.14%). Nine out of 13 interventions were carried out in a complete intracorporeal fashion, while conversion to open surgery was needed in 4 cases. Vascular complications involving the major blood vessels comprised of one case of inferior vena cava (IVC) tear. Digestive tract-related complications comprised two fistulas of the descending colon and one peritoneal breach. Multiorgan resection was performed in 6 cases.
Conclusion
Total nephrectomy in cases of XGPN and pyonephrosis is a challenging procedure. The laparoscopic approach is feasible, as most complications are resolved intracorporeally. However, it may remain reserved for large-volume centers with experienced surgeons.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


