{"title":"Hiperlactacidemia en pacientes con estatus asmático. Análisis mediante el modelo de Stewart","authors":"","doi":"10.1016/j.redar.2023.10.004","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Patients with status asthmaticus (SA) frequently present with lactic acidosis (LA). Our goal is to identify the nature of LA using the Stewart physicochemical model and to identify the independent factors associated with LA in children with SA.</p></div><div><h3>Methods</h3><p>Analytical study of a retrospective cohort using a nested case-control design. Twenty-eight episodes of SA in 24 children were included. Patients admitted to a paediatric intensive care unit (PICU) for SA over a 9-year period were recruited consecutively. LA was analysed using the Stewart model and the Strong Ion Calculator. Data and were analysed using descriptive statistics and regression models were fitted in the general linear model.</p></div><div><h3>Results</h3><p>Hyperlacticaemia (Lact[mM/L]<!--> <!-->=<!--> <!-->3.905 [95% <span>C</span>I<!--> <!-->=<!--> <!-->3.018-4.792]) and acidosis (pH<!--> <!-->=<!--> <!-->7.294 [95% CI<!--> <!-->=<!--> <!-->7.241-7.339]) were observed in 18 episodes (15 patients; 62.5%). According to the Stewart model, acidosis was caused by a decrease in strong ion difference. Initially, pCO2 was high (pCO2[mmHg]<!--> <!-->=<!--> <!-->45.806 [95% CI<!--> <!-->=<!--> <!-->37.314-54.298]) but the net unmeasured ion (NUI) component was normal (NUI<!--> <!-->=<!--> <!-->-4,461 [95% CI<!--> <!-->=<!--> <!-->-3.51 - -5.412]), and neither changed significantly over the clinical course. There was no need to determine pyruvate, as the NUI was normal and the LA was type B (non-hypoxic, lactate / pyruvate <<!--> <!-->25). We observed a correlation (p<!--> <!-->=<!--> <!-->0.023) between LA and intramuscular epinephrine administered on arrival at hospital, but not between LA and the cumulative dose of nebulized salbutamol.</p></div><div><h3>Conclusions</h3><p>Most patients with SA presented LA. The Stewart model confirmed that LA is not hypoxic, probably due to sympathomimetic-related glycolysis.</p></div>","PeriodicalId":46479,"journal":{"name":"Revista Espanola de Anestesiologia y Reanimacion","volume":"71 7","pages":"Pages 501-505"},"PeriodicalIF":0.9000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista Espanola de Anestesiologia y Reanimacion","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0034935624000094","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Patients with status asthmaticus (SA) frequently present with lactic acidosis (LA). Our goal is to identify the nature of LA using the Stewart physicochemical model and to identify the independent factors associated with LA in children with SA.
Methods
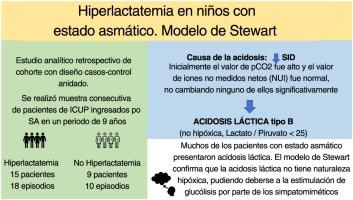
Analytical study of a retrospective cohort using a nested case-control design. Twenty-eight episodes of SA in 24 children were included. Patients admitted to a paediatric intensive care unit (PICU) for SA over a 9-year period were recruited consecutively. LA was analysed using the Stewart model and the Strong Ion Calculator. Data and were analysed using descriptive statistics and regression models were fitted in the general linear model.
Results
Hyperlacticaemia (Lact[mM/L] = 3.905 [95% CI = 3.018-4.792]) and acidosis (pH = 7.294 [95% CI = 7.241-7.339]) were observed in 18 episodes (15 patients; 62.5%). According to the Stewart model, acidosis was caused by a decrease in strong ion difference. Initially, pCO2 was high (pCO2[mmHg] = 45.806 [95% CI = 37.314-54.298]) but the net unmeasured ion (NUI) component was normal (NUI = -4,461 [95% CI = -3.51 - -5.412]), and neither changed significantly over the clinical course. There was no need to determine pyruvate, as the NUI was normal and the LA was type B (non-hypoxic, lactate / pyruvate < 25). We observed a correlation (p = 0.023) between LA and intramuscular epinephrine administered on arrival at hospital, but not between LA and the cumulative dose of nebulized salbutamol.
Conclusions
Most patients with SA presented LA. The Stewart model confirmed that LA is not hypoxic, probably due to sympathomimetic-related glycolysis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


