{"title":"Giant-cell arteritis with toothache","authors":"Jun Usami MD, PhD","doi":"10.1002/jgf2.684","DOIUrl":null,"url":null,"abstract":"<p>A 78-year-old woman visited the outpatient clinic with a 4-week history of low-grade fever of unknown origin. One week after fever onset, she visited the dental clinic because of upper left toothache and left jaw claudication, and she was scheduled to have a mouthpiece made. No dental caries was observed. Since the cause of fever was not clear, the patient visited our clinic. On presentation, she was alert, and her vital signs were normal. Physical examination revealed a slightly enlarged left temporal artery without pulsation and tenderness (Figure 1A). She did not complain of pain and morning stiffness about the shoulders, neck, hip girdle, and proximal thighs. There were no complications of polymyalgia rheumatica. Her C-reactive protein level was 4.8 mg/dL (reference: 0–0.3 mg/dL), and erythrocyte sedimentation rate was 85 mm/h (reference: 0–10 mm/h). Ultrasonography revealed thickened walls in both the temporal artery frontal branches (Figure 1B; left temporal artery). Giant-cell arteritis (GCA) was considered likely.<span><sup>1</sup></span> Left temporal artery biopsy was performed, which revealed a highly narrowed lumen. Lymphocytes, neutrophil infiltration, and granulation tissue formation were observed in the blood vessel wall, and multinucleated giant cells were also observed. The biopsy results confirmed the diagnosis, and 40 mg prednisolone (1 mg/kg body weight) was orally administered daily.<span><sup>1</sup></span> Symptoms resolved within a week.</p><p>Giant-cell arteritis is a vasculitis that often affects medium- and large-sized arteries and shows a variety of clinical manifestations (Table 1). Headache is present in over 80% of cases in a report.<span><sup>2</sup></span> Our patient complained of toothache, but she had no problems with her teeth. Giant-cell arteritis can also cause serious risks, such as blindness,<span><sup>3</sup></span> and requires prompt diagnosis. Giant-cell arteritis occurs less often in Japan, Korea, and other Asian countries than in Western countries; the reason for this discrepancy remains unclear. In Asian countries, GCA is one of the cause of fever of unknown origin. In primary care settings, the possibility of GCA should be considered in elderly Asian patients suffering from fever and pain in the temple; ultrasonography should be performed to detect wall thickening in the temporal artery frontal branches. This easy method is very useful for the diagnosis of this emergent disease.</p><p>None.</p><p>No potential conflict of interest relevant to this article was reported.</p><p>None.</p><p>We obtained informed consent from the patient for this case report.</p><p>None.</p>","PeriodicalId":51861,"journal":{"name":"Journal of General and Family Medicine","volume":"25 3","pages":"162-163"},"PeriodicalIF":1.8000,"publicationDate":"2024-03-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jgf2.684","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of General and Family Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jgf2.684","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
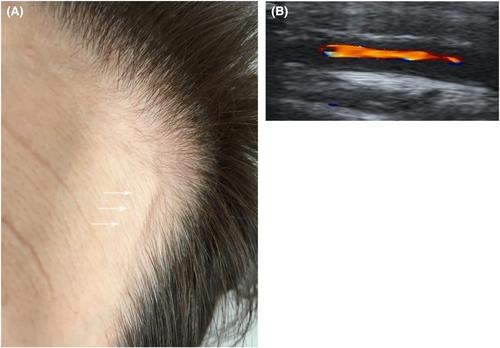
A 78-year-old woman visited the outpatient clinic with a 4-week history of low-grade fever of unknown origin. One week after fever onset, she visited the dental clinic because of upper left toothache and left jaw claudication, and she was scheduled to have a mouthpiece made. No dental caries was observed. Since the cause of fever was not clear, the patient visited our clinic. On presentation, she was alert, and her vital signs were normal. Physical examination revealed a slightly enlarged left temporal artery without pulsation and tenderness (Figure 1A). She did not complain of pain and morning stiffness about the shoulders, neck, hip girdle, and proximal thighs. There were no complications of polymyalgia rheumatica. Her C-reactive protein level was 4.8 mg/dL (reference: 0–0.3 mg/dL), and erythrocyte sedimentation rate was 85 mm/h (reference: 0–10 mm/h). Ultrasonography revealed thickened walls in both the temporal artery frontal branches (Figure 1B; left temporal artery). Giant-cell arteritis (GCA) was considered likely.1 Left temporal artery biopsy was performed, which revealed a highly narrowed lumen. Lymphocytes, neutrophil infiltration, and granulation tissue formation were observed in the blood vessel wall, and multinucleated giant cells were also observed. The biopsy results confirmed the diagnosis, and 40 mg prednisolone (1 mg/kg body weight) was orally administered daily.1 Symptoms resolved within a week.
Giant-cell arteritis is a vasculitis that often affects medium- and large-sized arteries and shows a variety of clinical manifestations (Table 1). Headache is present in over 80% of cases in a report.2 Our patient complained of toothache, but she had no problems with her teeth. Giant-cell arteritis can also cause serious risks, such as blindness,3 and requires prompt diagnosis. Giant-cell arteritis occurs less often in Japan, Korea, and other Asian countries than in Western countries; the reason for this discrepancy remains unclear. In Asian countries, GCA is one of the cause of fever of unknown origin. In primary care settings, the possibility of GCA should be considered in elderly Asian patients suffering from fever and pain in the temple; ultrasonography should be performed to detect wall thickening in the temporal artery frontal branches. This easy method is very useful for the diagnosis of this emergent disease.
None.
No potential conflict of interest relevant to this article was reported.
None.
We obtained informed consent from the patient for this case report.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


