{"title":"Is multidisciplinary treatment effective for invasive intraductal papillary mucinous carcinoma?","authors":"Seiko Hirono, Ryota Higuchi, Goro Honda, Satoshi Nara, Minoru Esaki, Naoto Gotohda, Hideki Takami, Michiaki Unno, Teiichi Sugiura, Masayuki Ohtsuka, Yasuhiro Shimizu, Ippei Matsumoto, Toshifumi Kin, Hiroyuki Isayama, Daisuke Hashimoto, Yasuji Seyama, Hiroaki Nagano, Kenichi Hakamada, Satoshi Hirano, Yuichi Nagakawa, Shugo Mizuno, Hidenori Takahashi, Kazuto Shibuya, Hideki Sasanuma, Taku Aoki, Yuichiro Kohara, Toshiki Rikiyama, Masafumi Nakamura, Itaru Endo, Yoshihiro Sakamoto, Akihiko Horiguchi, Takashi Hatori, Hirofumi Akita, Toshiharu Ueki, Tetsuya Idichi, Keiji Hanada, Shuji Suzuki, Keiichi Okano, Hiromitsu Maehira, Fuyuhiko Motoi, Yasuhiro Fujino, Satoshi Tanno, Akio Yanagisawa, Yoshifumi Takeyama, Kazuichi Okazaki, Sohei Satoi, Hiroki Yamaue","doi":"10.1002/ags3.12790","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Surgical resection is standard treatment for invasive intraductal papillary mucinous carcinoma (IPMC); however, impact of multidisciplinary treatment on survival including postoperative adjuvant therapy (AT), neoadjuvant therapy (NAT), and treatment for recurrent lesions is unclear. We investigated the effectiveness of multidisciplinary treatment in prolonging survival of patients with invasive IPMC.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This retrospective multi-institutional study included 1183 patients with invasive IPMC undergoing surgery at 40 academic institutions. We analyzed the effects of AT, NAT, and treatment for recurrence on survival of patients with invasive IPMC.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Completion of the planned postoperative AT for 6 months improved the overall survival (OS), disease-specific survival (DSS), and recurrence-free survival (RFS) of patients with stage IIB and stage III resected invasive IPMC, elevated preoperative carbohydrate antigen 19–9 level, lymphovascular invasion, perineural invasion, serosal invasion, and lymph node metastasis on un-matched and matched analyses. Of the patients with borderline resectable (BR) invasive IPMC, the OS (<i>p</i> = 0.001), DSS (<i>p</i> = 0.001), and RFS (<i>p</i> = 0.001) of patients undergoing NAT was longer than that of those without on the matched analysis. Of the 484 invasive IPMC patients (40.9%) who developed recurrence after surgery, the OS of 365 patients who received any treatment for recurrence was longer than that of those without treatment (40.6 vs. 22.4 months, <i>p</i> < 0.001).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Postoperative AT might benefit selected patients with invasive IPMC, especially those at high risk of poor survival. NAT might improve the survivability of BR invasive IPMC. Any treatment for recurrence after surgery for invasive IPMC might improve survival.</p>\n </section>\n </div>","PeriodicalId":8030,"journal":{"name":"Annals of Gastroenterological Surgery","volume":"8 5","pages":"845-859"},"PeriodicalIF":2.9000,"publicationDate":"2024-03-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ags3.12790","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterological Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12790","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Surgical resection is standard treatment for invasive intraductal papillary mucinous carcinoma (IPMC); however, impact of multidisciplinary treatment on survival including postoperative adjuvant therapy (AT), neoadjuvant therapy (NAT), and treatment for recurrent lesions is unclear. We investigated the effectiveness of multidisciplinary treatment in prolonging survival of patients with invasive IPMC.
Methods
This retrospective multi-institutional study included 1183 patients with invasive IPMC undergoing surgery at 40 academic institutions. We analyzed the effects of AT, NAT, and treatment for recurrence on survival of patients with invasive IPMC.
Results
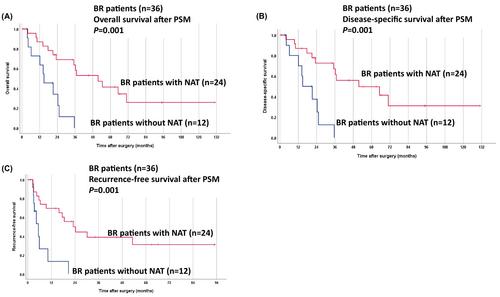
Completion of the planned postoperative AT for 6 months improved the overall survival (OS), disease-specific survival (DSS), and recurrence-free survival (RFS) of patients with stage IIB and stage III resected invasive IPMC, elevated preoperative carbohydrate antigen 19–9 level, lymphovascular invasion, perineural invasion, serosal invasion, and lymph node metastasis on un-matched and matched analyses. Of the patients with borderline resectable (BR) invasive IPMC, the OS (p = 0.001), DSS (p = 0.001), and RFS (p = 0.001) of patients undergoing NAT was longer than that of those without on the matched analysis. Of the 484 invasive IPMC patients (40.9%) who developed recurrence after surgery, the OS of 365 patients who received any treatment for recurrence was longer than that of those without treatment (40.6 vs. 22.4 months, p < 0.001).
Conclusion
Postoperative AT might benefit selected patients with invasive IPMC, especially those at high risk of poor survival. NAT might improve the survivability of BR invasive IPMC. Any treatment for recurrence after surgery for invasive IPMC might improve survival.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


